Introduction
Ectopic pregnancy (EP) is defined as a pregnancy that occurs outside the uterine cavity, most commonly in the ampullary portion of the fallopian tube [1]. Twin ectopic pregnancy (TEP) is exceedingly rare, particularly when it occurs spontaneously and both embryos are implanted within the same tube. Because the risk of tubal rupture is higher than in singleton EP, early diagnosis is critical. Owing to its exceptional rarity, no specific management or treatment guidelines have been established.
Case report
A 30-year-old primigravida presented to the Emergency Department with vaginal bleeding, hypogastric pain, and 7 weeks of amenorrhea. She reported no relevant medical or surgical history and no additional symptoms. On physical examination, hypogastric tenderness was noted on deep abdominal palpation, without signs of peritoneal irritation. Vital signs were stable. Pelvic examination revealed a closed cervix and tenderness in the right adnexal region.
Laboratory testing showed a serum β-subunit of human chorionic gonadotropin (β-hCG) level of 56,172 mIU/mL. All other laboratory parameters were within normal limits. Transvaginal ultrasound demonstrated an empty uterus with an endometrial thickness of 9 mm. A 40 × 38 mm anechoic image, consistent with a corpus luteum, was identified in the left ovary, while the right ovary had a normal ultrasound appearance. Adjacent to the right ovary, two gestational sacs were visualized, each containing an embryo with a crown–rump length of 8.9 mm and 8.8 mm, corresponding to 6 weeks and 6 days of gestation. Cardiac activity was detected in both embryos (Figure 1).
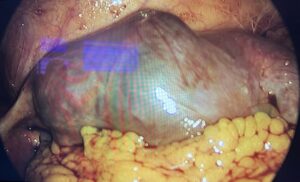
The patient was diagnosed with a unilateral tubal twin pregnancy. The findings and available therapeutic options were discussed, and laparoscopic surgical management was selected. The procedure was performed using a 12-mm umbilical trocar and two 5-mm accessory trocars placed in the left iliac region. Intraoperatively, a right adnexal mass was identified, corresponding to a tubal lesion measuring approximately 84 × 45 mm (Figure 2). After careful inspection of the entire abdominal cavity, a right salpingectomy was performed (Figures 3 and 4) without complications. The surgical specimen was retrieved in a closed extraction bag through the umbilical trocar and sent for histopathological examination. The postoperative course was uneventful, and the patient was discharged 12 hours after surgery. Histopathological analysis confirmed a tubal TEP, identifying two embryos.
Discussion
A literature review was conducted using a predefined search strategy. The databases PubMed/MEDLINE, Scopus, Embase, and ScienceDirect were searched using the following terms: (“unilateral tubal twin ectopic pregnancy” OR “unilateral twin tubal pregnancy” OR “spontaneous live unilateral tubal twin ectopic pregnancy”) NOT (heterotopic), without time restrictions. Clinical case reports, case series, and review articles were included.
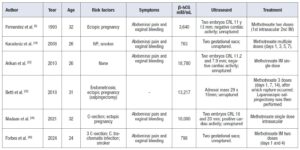
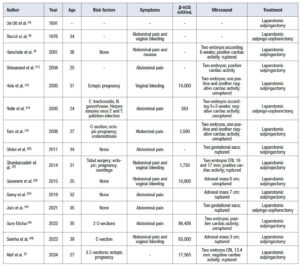
A total of 82 articles were initially identified. After duplicate removal using Zotero Reduplicator and additional manual screening, 45 articles met the eligibility criteria. The main clinical characteristics extracted from these studies are summarized in Tables 1, 2, 3, and 4, categorized according to therapeutic approach: medical management, laparoscopy, laparotomy, or unspecified treatment.
The incidence of EP has increased in recent years, largely due to the growing prevalence of risk factors such as pelvic inflammatory disease, prior pelvic surgery, and the use of assisted reproductive techniques [3]. Tubal implantation remains the most common location, accounting for more than 90% of cases [23]. In contrast, TEP are exceptionally rare, with an estimated incidence of approximately 1 in 125,000 spontaneous pregnancies [1]. The presence of fetal cardiac activity in both embryos represents an even more unusual clinical finding.
TEP are associated with higher morbidity and mortality than singleton EP, particularly when both embryos are located within the same fallopian tube. The increased tubal distension results in a substantially higher risk of rupture, reported in 30–50% of cases [2].
The first documented description of a unilateral TEP dates back to 1891 [4]. Nearly a century later, the introduction of ultrasonography made preoperative diagnosis of this rare condition possible [7].
Most reported cases involve young women, with a mean age of 31.9 ± 5.99 years (range 24–51 years). Among the published cases, identifiable risk factors were present in 22 of 46 patients (47.8%). The most frequently reported risk factors included a history of pelvic surgery (notably cesarean section), previous EP, pelvic inflammatory disease, and the use of assisted reproductive techniques.
Abdominal pain was the most common presenting symptom, reported in all cases, followed by vaginal bleeding. Owing to the larger size of TEP, symptoms and complications—particularly tubal rupture—tend to occur earlier, leading to diagnosis most frequently after 6–7 weeks of amenorrhea. In this series, the latest diagnosis was reported at 12 weeks [33].
Serum β-hCG levels were generally higher than expected for the corresponding gestational age. However, this parameter showed wide interindividual variability and should therefore be interpreted with caution [47,48].
Transvaginal ultrasound was the most useful imaging modality for determining the location of the pregnancy, with a reported sensitivity of 87–99% and specificity of 94–99% [2]. Nevertheless, visualization of two embryos was not always possible, and in some cases the diagnosis of unilateral TEP was established only postoperatively through histopathological examination of the surgical specimen [34]. The combined use of transvaginal ultrasound and β-hCG measurement has substantially improved the diagnostic accuracy for EP, even in rare presentations such as TEP.
This review did not identify any preference for right- or left-sided tubal involvement, with both sides reported at similar frequencies.
Regarding management, because of the extremely low incidence of spontaneous unilateral tubal TEP, no standardized therapeutic protocol exists [49]. The choice of treatment approach was mainly determined by the patient’s hemodynamic stability, prior surgical history, and/or surgeon preference.
Overall, surgical management was far more common than medical treatment (40 cases vs. 5 cases in this series). Salpingectomy was the most frequently performed procedure, via either laparotomy or laparoscopy. Laparotomy was used in 17 cases, while laparoscopy was performed in 23 cases (one case was not specified). Despite the increasing trend toward minimally invasive surgery, laparotomy remains the preferred approach in cases of tubal rupture, hemodynamic instability, or based on the surgeon’s judgment.
Although alternative surgical techniques have been successfully used for singleton EP, their effectiveness in TEP has not been adequately studied.
In hemodynamically stable patients without medical comorbidities that contraindicate methotrexate (MTX), such as liver or kidney disease [3], and with no signs of tubal rupture, medical management with MTX has been attempted. In the present series, six cases were treated with MTX; however, one of these subsequently required surgical intervention due to tubal rupture [32].
Overall prognosis depends largely on early diagnosis and prompt management, with most reported cases showing favorable maternal outcomes. The principal risk remains tubal rupture with severe hemorrhage. Therefore, it is essential to recognize the increased risk associated with suspected unilateral tubal TEP and to manage these cases proactively and appropriately.
Highlights
- TEP is a rare condition, but one that must be considered due to the higher risk of rupture.
- A warning sign of a TEP is the finding of unexpectedly high β-hCG levels.
- Difficulty in identifying both embryos through ultrasound may occur.
- There are no standardized treatment recommendations; surgical approach is most commonly chosen.
Conclusion
Spontaneous unilateral tubal TEP is an extremely rare condition and may be associated with significant maternal morbidity if not promptly recognized and treated. It should be suspected in the presence of pelvic pain, abnormally elevated β-hCG levels, and suggestive ultrasound findings, even in the absence of classic risk factors for EP. Management should be individualized, with surgical treatment remaining the preferred approach, although selected cases have been successfully managed medically. The development of evidence-based guidelines derived from the existing scientific literature is essential to improve diagnosis, management, and outcomes in these rare cases.
Author contributions
Sandra Borja-Vergel performed the literature review and wrote the manuscript.
José Olmedilla-Bahillo and María Martín-Gómez literature review and revision of the manuscript.
Sandra Borja-Vergel, Sonia M. García-García, and Paula Parrondo-Sánchez contributed to patient care, data acquisition and interpretation, and selection of the histopathological images included in the manuscript.
María J. Cancelo-Hidalgo contributed to drafting the manuscript and critically revising the article for important intellectual content.
All authors approved the final submitted manuscript.
Patient Consent
Informed consent was obtained from the patient. Institutional approval was not required for publication of this case report.