Introduction
Ovarian torsion is a gynecologic emergency characterized by partial or complete rotation of the ovary around its vascular pedicle, leading to compromised blood flow and potential ovarian ischemia [1]. It accounts for approximately 2.7% of all gynecologic emergencies [2] and predominantly affects women of reproductive age, typically in association with ovarian cysts, adnexal masses, or hyperstimulation during fertility treatments [3]. The occurrence of ovarian torsion in postmenopausal women is rare [4] due to the reduced size and diminished functional activity of the ovaries after menopause. Bilateral ovarian torsion is an even more infrequent phenomenon, with limited cases documented in the literature [5]. In postmenopausal women, the pathophysiology of ovarian torsion may differ from that observed in younger women. Although ovarian masses remain contributing factors, other predisposing conditions include pelvic adhesions, previous abdominal or pelvic surgeries, and increased ovarian mobility due to atrophy of supportive ligaments. The clinical presentation can be nonspecific, often mimicking other acute abdominal pathologies. Common symptoms include the acute onset of severe lower abdominal pain, nausea, vomiting, and sometimes low-grade fever [6]. This nonspecific symptomatology may delay diagnosis and increase the risk of ovarian necrosis. Timely recognition of ovarian torsion is critical because prolonged torsion can lead to irreversible ischemic damage, infarction, and, ultimately, necrosis of the ovary. Diagnostic tools, particularly ultrasonography with Doppler imaging, play a central role in the detection and evaluation of adnexal torsion. Surgical exploration remains the definitive diagnostic and therapeutic approach. This case report aims to contribute to the limited body of literature on bilateral ovarian torsion in postmenopausal women and to emphasize the importance of maintaining a broad differential diagnosis when evaluating acute abdominal pain in this population.
Case report
A 52-year-old postmenopausal woman with no significant medical or surgical history presented to the emergency department with a 24-hour history of sudden-onset severe lower abdominal pain, associated with nausea and vomiting. She denied fever, vaginal bleeding, or urinary symptoms. Menopause had occurred at age 50, and her gynecologic history was otherwise unremarkable.
On examination, she was afebrile (temperature 36.7°C), with stable vital signs (blood pressure 135/85 mmHg, heart rate 92 bpm). She appeared in distress due to pain. Abdominal palpation revealed diffuse tenderness, most notable in the lower quadrants, with guarding but no palpable masses.
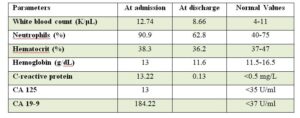
Laboratory results showed mild leukocytosis (white blood cell count 12,740/μL), with normal hemoglobin and electrolyte levels. CA 19-9 was elevated (Table 1).
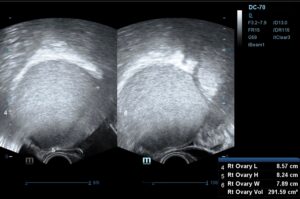
Transvaginal ultrasonography revealed a large, unilocular cyst, with hyperechogenic content, without internal septations or papillary projections, measuring 8.57 × 8.24 × 7.89 cm, possibly originating from the right adnexa (Figure 1). Transabdominal ultrasonography revealed two thin-walled cystic masses with smooth borders and mixed echogenic content, measuring 11.28 x 5.82 x 10.34 cm, which appeared to arise from the adnexa (Figure 2), and, according to IOTA simple rules, were presumed benign.
Features suggestive of an atypical mature cystic teratoma (dermoid cyst) were identified, including diffuse linear hyperechogenicities (corresponding to hair), a Rokitansky nodule, and posterior acoustic shadowing. This cyst was also presumed benign, according to the simple rules of IOTA (unilocular with acoustic shadowing and no features of malignancy).
Using the IOTA ADNEX calculator, the following risks were calculated: probability of benign ovarian tumour: 98.8%; risk of malignant ovarian tumour: 1.2%; risk of borderline ovarian tumour: 0.5%; risk of stage I ovarian tumour: 0.6%; risk of stage II–IV ovarian tumour: 0.1%; risk of metastatic ovarian tumour: 0.1%. No free intraperitoneal fluid was identified.
The findings were highly suggestive of large, bilateral, likely benign ovarian cysts with clinical features of torsion.
The patient was taken emergently for exploratory laparotomy. Intraoperative findings confirmed bilateral ovarian torsion, with each ovary twisted more than 720° around its pedicle and exhibiting marked enlargement. No ascites, peritoneal implants, or signs of malignancy were observed. Bilateral salpingo-oophorectomy was performed.
Histopathological examination confirmed hemorrhagic infarction of both ovaries with areas of necrosis and no evidence of malignancy. Each ovary contained a mature cystic teratoma composed of well-differentiated ectodermal elements, including skin, hair, and sebaceous glands. The fallopian tubes were unremarkable. Cytological analysis of the peritoneal lavage showed no evidence of malignancy.
The postoperative course was uncomplicated. The patient was discharged on postoperative day 3 and remained asymptomatic at her two-week follow-up.
Discussion
Ovarian torsion is a time-sensitive diagnosis that requires a high index of suspicion, particularly in atypical patient populations such as postmenopausal women. In most cases, ovarian torsion is unilateral and occurs in the setting of ovarian cysts or masses. Bilateral torsion is extremely rare, with only a few documented cases in the literature, and presents a greater diagnostic challenge due to the atypical presentation in postmenopausal patients [7]. The nonspecific symptoms, including abdominal pain, nausea, and vomiting, can mimic other acute abdominal conditions such as cystitis, appendicitis, diverticulitis, or bowel obstruction, leading to potential diagnostic delays. Several case reports have demonstrated how ovarian torsion may present with misleading clinical features in older patients. For instance, torsion associated with an ovarian teratoma has been reported to mimic small bowel obstruction in an elderly woman [8], while in another case, chronic torsion was initially mistaken for a subserosal fibroid in a postmenopausal patient [9]. These examples highlight the need to consider ovarian torsion in the differential diagnosis of acute or subacute pelvic pain, regardless of age.
The pathophysiology of ovarian torsion involves venous congestion and arterial occlusion due to twisting of the adnexal structures. This leads to ischemia and, if not promptly corrected, ovarian necrosis.
Imaging, particularly ultrasonography with Doppler, plays a crucial role in the diagnostic workup of ovarian torsion by assessing the ovarian size (an increase in ovarian size with a mean maximum diameter of 80 mm is expected due to stromal edema), the echotexture (follicular displacement to the periphery of the ovary accompanied by a follicular ring sign can be observed in 40% of the cases, which is considered an early sign of torsion), the presence of free fluid to the Douglas pouch (70%), the tenderness when the probe touches the torted adnexa (80%) and the vascular flow (whirlpool sign and progressive loss of the ovarian blood flow first of the veins, followed by the arteries). However, the absence of Doppler abnormalities does not exclude torsion, as intermittent twisting may preserve arterial perfusion despite venous obstruction [10]. Cross-sectional imaging, such as computed tomography (CT) or magnetic resonance imaging (MRI), can provide additional information in uncertain cases [11].
Laparoscopy is the preferred approach for adnexal surgery in stable patients, offering less postoperative pain, shorter hospitalization, faster recovery, and lower morbidity compared with laparotomy. Its safety and efficacy in benign adnexal disease and bilateral salpingo-oophorectomy are well established [12]. Nevertheless, laparotomy remains appropriate in selected cases, such as suspected malignancy, very large masses, extensive adhesions, or inadequate visualization. In our case, laparotomy was chosen due to the large ovarian cysts and the high risk of intra-abdominal spillage with a laparoscopic approach. The choice of surgical approach should be guided by thorough preoperative assessment, taking into account the clinical setting, the surgeon’s expertise, and the patient’s preferences [13].
In postmenopausal women, the reduced functional role of the ovaries and the increased risk of malignancy, along with the risk of ovarian necrosis, peritonitis, recurrence of torsion, and the potential need for repeat surgery, often justify more definitive surgical management, such as salpingo-oophorectomy, rather than conservative detorsion [14]. Bilateral salpingo-oophorectomy is typically recommended, particularly when both ovaries appear necrotic or when the underlying etiology is uncertain [15]. In contrast, in premenopausal women, more conservative management may be considered due to the potential long-term consequences of oophorectomy; indeed, an observational study by Cusimano et al. reported that bilateral salpingo-oophorectomy performed during non-malignant hysterectomy was associated with increased all-cause mortality in women under 50 years of age, whereas no such association was observed in women aged 50 years or older [16].
In contrast, the management in women of reproductive age focuses on ovarian preservation, whenever possible, to maintain fertility [17]. Conservative detorsion is the preferred approach, even in cases of prolonged torsion, as studies have shown that ovarian function can often recover despite apparent ischemia [18]. Laparoscopic detorsion, with or without cystectomy, is the gold standard in younger women, aiming to restore ovarian perfusion and minimize long-term reproductive sequelae [19]. However, in postmenopausal women, the risk-benefit balance shifts due to the diminished importance of ovarian hormonal function and the increased concern for malignancy.
This case underscores the importance of bearing in mind that acute gynecological pathologies should not be automatically eliminated from the differential diagnosis in menopause and that prompt surgical intervention in suspected ovarian torsion is the only way to prevent complications such as necrosis, infection, and peritonitis. It also highlights the differences in management strategies between postmenopausal women and women of reproductive age, reflecting the differing priorities of ovarian conservation versus malignancy risk reduction.
In conclusion, bilateral ovarian torsion is an extremely rare and potentially life-threatening condition that requires prompt recognition and management. This case report emphasizes the importance of maintaining a high index of suspicion for ovarian torsion in postmenopausal women presenting with acute pelvic pain, despite its rarity in this population. Early surgical intervention is critical to prevent irreversible ischemic damage and associated complications such as necrosis and peritonitis. The management approach in postmenopausal women typically prioritizes definitive surgical treatment, such as bilateral salpingo-oophorectomy, due to the reduced functional importance of the ovaries and the increased risk of underlying malignancy. This differs from the approach in reproductive-age women, where ovarian conservation is often feasible and desirable to preserve fertility. Understanding these differences can aid clinicians in making patient-centered, evidence-based management decisions. Ultimately, this case contributes to the growing body of literature on adnexal torsion and highlights the need for increased awareness and timely diagnosis to improve clinical outcomes in both postmenopausal and reproductive-age populations.
Author contributions
Maria Ntioudi and Georgios Varveris participated in conceptualization, investigation, methodology, writing and original drafting the manuscript. Vasiliadou Katerina was responsible for investigation, methodology and reviewing the paper. Diamantopoulou Alexandra participated in supervision, reviewing and validating the final document.
Ethical statement
Written informed consent was obtained from the patient for the publication of this case report.