Introduction
Congenital uterine anomalies (CUA) result from abnormal embryonic development of the Müllerian ducts. These defects may lead to agenesis (partial or complete) of the ducts, incomplete or absent development of one duct, partial or total failure of midline fusion, or defects in reabsorption of the intermüllerian septum [1,2]. CUA are present in 1–10% of women in the general population, 2–8% of infertile women, and 5–30% of women with a history of miscarriage [3–5].
According to the consensus of the European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE), CUA are classified into classes and subclasses based on anatomy, embryological origin, anatomical variations, and increasing severity. Class U0 represents a normal uterus, whereas class U5 refers to an aplastic uterus, with or without a rudimentary cavity. Intermediate classes include dysmorphic uterus (U1), septate uterus (U2), bicorporal uterus (U3), and hemi-uterus (U4) [6]. CUA may contribute to infertility and obstetric complications, including spontaneous abortion, preterm delivery, malpresentation, and fetal growth restriction (FGR) [3–5].
The septate uterus results from a canalization defect characterized by incomplete resorption of the midline septum. It is defined by a normal external uterine contour and an internal fundal indentation exceeding 50% of the uterine wall thickness, forming a septum that may be partial (above the level of the cervix) or complete (reaching the cervix) [6]. To better differentiate it from an arcuate uterus, some authors define the septum as longer than 1.5 cm, with its central point forming an acute angle [7]. The septate uterus has been associated with many of the complications described above. A systematic review reported decreased clinical pregnancy [odds ratio (OR) 0.45; 95% confidence interval (CI) 0.21–0.95] and live birth (OR 0.25; 95% CI 0.09–0.75) rates, as well as increased risks of first-trimester (OR 2.55; 95% CI 1.33–4.91) and second-trimester miscarriage (OR 4.33; 95% CI 2.52–7.43), preterm delivery (OR 2.93; 95% CI 2.01–4.28), malpresentation (OR 11.49; 95% CI 5.24–25.17), cesarean delivery (OR 4.84; 95% CI 2.33–10.02), and perinatal mortality (OR 2.57; 95% CI 1.08–6.08) [8]. In this review, the risk of FGR was not increased, in contrast to another meta-analysis that reported a higher risk of FGR (OR 2.54; 95% CI 1.04–6.23) [5]. Hysteroscopic septoplasty appears to reduce the miscarriage rate from 80% to 15% [9].
Bicorporeal uterus and hemi-uterus result from unification defects. The bicorporeal uterus arises from failure of fusion of the Müllerian ducts and is characterized by an external midline fundal indentation exceeding 50% of the uterine wall thickness, resulting in two partially or completely separate uterine hemicavities [6]. Clinical pregnancy and live birth rates do not appear to be significantly affected; however, the risk of obstetric complications is increased, particularly preterm delivery (OR 3.69; 95% CI 2.6–5.22), malpresentation (OR 10.87; 95% CI 6.68–17.68), cesarean delivery (OR 5.23; 95% CI 2.11–10.02), FGR (OR 2.84; 95% CI 1.68–4.8), and perinatal mortality (OR 3.17; 95% CI 2.08–4.84) [8].
Incomplete or absent development of one Müllerian duct results in a hemi-uterus, a unilateral uterine cavity [6]. Hemi-uterus has been associated with decreased clinical pregnancy (OR 0.75; 95% CI 0.58–0.99) and live birth (OR 0.57; 95% CI 0.34–0.96) rates, as well as an increased risk of preterm delivery (OR 2.83; 95% CI 1.92–4.19), malpresentation (OR 8.09; 95% CI 3.14–20.84), and FGR (OR 3.5; 95% CI 1.24–9.91) [8]. In contrast, Simsek et al. reported comparable live birth rates when women with hemi-uterus were compared with controls [10].
Recent studies suggest that CUA may negatively influence the outcomes of in vitro fertilization (IVF) [2–11], but the etiology and underlying mechanisms remain unclear. Many studies are limited by the absence of standardized control groups, variability in diagnostic methodologies, lack of prospective randomized trials, and potential selection bias. Additionally, the impact of surgical correction remains debatable. Therefore, we aimed to describe the prevalence and classification of CUA in a population of infertile women and to analyze reproductive outcomes and obstetric complications in comparison with a control group.
Methods
Study design, setting, and participants
We conducted a retrospective cohort study at the Reproductive Medicine Unit of a university hospital between January 2014 and December 2023. The study group included women with CUA. Using the keywords “septate uterus,” “unicornuate uterus,” “hemi-uterus,” “bicornuate uterus,” and “bicorporeal uterus” (in Portuguese), we retrieved clinical data from patients diagnosed with major CUA (classes U2–U4) during their initial infertility assessment. Dysmorphic and aplastic uteri were not included in this study [6]. For the control group, we retrieved clinical data from infertile women with a normal uterus by selecting the first four ART cycles performed each October during the study period.
Outcomes and measures
The primary outcomes were clinical pregnancy, confirmed by ultrasonographic detection of one or more gestational sacs, and live birth, defined as the delivery of a living fetus after 22 completed weeks of gestation [12]. Pregnancy and live birth rates were calculated per embryo transfer.
Secondary outcomes included the total number of oocytes and mature oocytes, the number of embryos, and the fertilization rate, defined as the sequence of biological processes initiated by the entry of a spermatozoon into a mature oocyte, resulting in the formation of pronuclei [12]. We also assessed ectopic pregnancy, defined as occurring outside the uterine cavity; first-trimester pregnancy loss, defined as spontaneous loss of an intrauterine pregnancy; preterm delivery, defined as occurring before 37 completed weeks but after 22 weeks of gestation; fetal growth restriction, defined as an estimated fetal weight below the tenth percentile for gestational age by prenatal ultrasound; low birth weight (LBW), defined as less than 2,500 g; and cesarean delivery [12,13].
Ethics declaration
This study was approved by the Ethics Committees of the Faculty of Medicine, University of Coimbra, and the Unidade Local de Saúde (ULS) de Coimbra. A waiver of informed consent was granted. All procedures involving human participants were conducted in accordance with ethical standards.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics, version 29 (New York, USA). Continuous data are presented as means ± standard deviation (SD) or medians with interquartile range (Q1–Q3). Categorical variables are presented as frequencies and percentages. Baseline characteristics and outcomes in the study and control groups were compared using independent hypothesis tests. Continuous variables were compared using the t-test, and categorical variables using the chi-squared or Fisher’s exact test, as appropriate. The level of statistical significance was set at α = 0.05.
Results
Participants
During the study period, 6,981 women underwent their first infertility assessment. According to the selected criteria, clinical data from 112 participants were analyzed, resulting in a CUA prevalence of 1.60%.
Reproductive outcomes were not statistically analyzed in participants (n = 62) who had not undergone ART for the following reasons: 16 achieved spontaneous pregnancy (descriptively analyzed); 5 underwent intrauterine insemination (descriptively analyzed); 8 reached the age limit (40 years) for treatment covered by the national health system; 4 sought counseling and fertility preservation in the context of oncological or other fertility-affecting conditions; and 29 dropped out or suspended treatment.
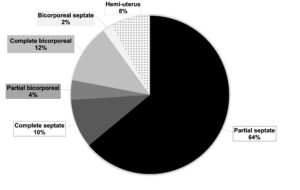
After these exclusions, 50 women with CUA were included in the study. Among them, 32 (64%) had a partial septate uterus, 5 (10%) a complete septate uterus, 2 (4%) a partial bicorporeal uterus, 6 (12%) a complete bicorporeal uterus, 1 (2%) a bicorporeal septate uterus, and 4 (8%) a hemi-uterus. Figure 1 illustrates the distribution of CUA subclasses. For the control group, after excluding women in whom a normal uterine cavity could not be confirmed, 40 women were included.
Baseline characteristics
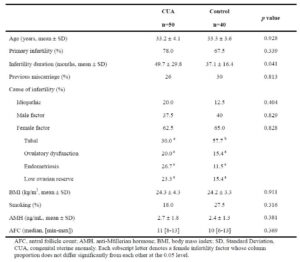
Baseline characteristics are presented in Table 1. The groups did not differ significantly in age, infertility type, previous miscarriages, body mass index (BMI), smoking prevalence, or ovarian reserve markers, including anti-Müllerian hormone (AMH) levels and antral follicle count (AFC). However, women with CUA had a longer duration of infertility (49.7 ± 29.8 vs. 37.1 ± 16.4 months, p = 0.041) and a lower proportion of tubal-factor infertility (30.0% vs. 57.7%).
Reproductive and obstetric outcomes
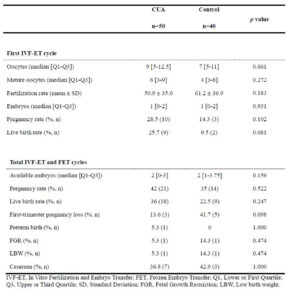
Reproductive and obstetric outcomes are presented in Table 2. In the first IVF and embryo transfer (IVF-ET) cycle, there were no significant differences between groups in the number of oocytes, fertilization rate, embryos available for transfer, or pregnancy and live birth rates.
No differences were observed after analysis of cumulative IVF-ET and frozen embryo transfer (FET) cycles. Women with CUA had similar numbers of embryos available for transfer, as well as comparable implantation, pregnancy, and live birth rates. They also showed no significant differences in first-trimester pregnancy loss, preterm delivery, fetal growth restriction, or cesarean delivery rates.
Despite these findings, the CUA group experienced two obstetric complications: one fetal death at 27 weeks and one medical termination of pregnancy at 17 weeks due to premature rupture of membranes, both in women with a partial septate uterus. No ectopic pregnancies were reported.
Subgroup analysis
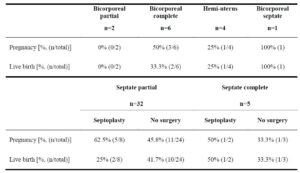
A descriptive analysis of the primary outcomes in the CUA group was performed and is presented in Tables 3 and 4. When considering the main CUA classes, women with a septate uterus had the best outcomes, whereas those with a hemi-uterus had the poorest.
No pregnancies occurred in the two women with a partial bicorporeal uterus. Among the six women with a complete bicorporeal uterus, three became pregnant, although only two had a live birth. The only woman diagnosed with a bicorporeal septate uterus had a live birth.
The pregnancy rate in the septate uterus group was 48.6%. Among the 32 women with a partial septate uterus who underwent ART cycles, 8 (25%) had hysteroscopic septoplasty, 7 of them before treatment. After resection, two pregnancies occurred in the first ART cycle: one resulted in a full-term live birth and the other in a spontaneous abortion. In subsequent cycles, three additional pregnancies were observed: one resulted in a full-term live birth, one in fetal death at 27 weeks of gestation, and one in medical termination of pregnancy due to premature rupture of membranes at 17 weeks. One patient underwent resection after two ART cycles without pregnancy but was lost to follow-up.
Among the 24 women (75%) who did not undergo septoplasty, three achieved pregnancy in the first ART cycle, all resulting in full-term deliveries. Across all cycles, eight additional pregnancies were recorded, leading to seven full-term deliveries and one spontaneous abortion.
Among the five women with a complete septate uterus, two (40%) underwent septoplasty before ART. Of these, one (50%) achieved pregnancy in the first ART cycle, resulting in a full-term birth, while no pregnancies occurred in subsequent cycles. Of the three women (60%) who did not undergo the procedure, one (33.3%) achieved clinical pregnancy in the first ART cycle, also resulting in a full-term birth.
Regarding outcomes after septoplasty compared with no surgical intervention, women with a partial septate uterus had a lower live birth rate (25% vs. 41.7%), whereas women with a complete septate uterus had a higher live birth rate (50% vs. 33.3%).
Spontaneous pregnancies
Among the initial population of women with CUA (n = 112), 16 (14%) achieved spontaneous pregnancy during the initial workup. Of these, 12 had a partial septate uterus, 3 had a complete septate uterus, and 1 had a complete bicorporeal uterus. Septoplasty was performed in 41.7% (5/12) of women with a partial septate uterus and in 33.3% (1/3) of those with a complete septate uterus.
Six women were lost to follow-up. Two women had two spontaneous pregnancies each, resulting in a total of 12 recorded live births. The woman with a bicorporeal uterus had one case of FGR. Among women with a complete septate uterus, records were available for only one, who did not undergo septoplasty and had a cesarean delivery. Among the five women with a partial septate uterus who underwent septoplasty, six deliveries were recorded, including one cesarean. Among those who did not undergo septoplasty, four deliveries were recorded, including one preterm birth and one cesarean delivery.
Identified causes of infertility included ovulatory dysfunction in 6.25% of women (1/16), idiopathic infertility in 43.7% (7/16), mixed factors in 37.5% (6/16), and male-related factors in 12.5% (2/16).
Intrauterine insemination
All women who underwent intrauterine insemination (n = 5) had a partial septate uterus, and none had a prior septoplasty. Three pregnancies (60%) occurred, resulting in two full-term deliveries and one spontaneous abortion.
Discussion
Our results showed that reproductive and obstetric outcomes in women with CUA were not different from those of the control group. The prevalence of major CUA (i.e. classes U2–U4; aplastic and dysmorphic uteri were not included) among women undergoing initial infertility evaluation was 1.60%. Some authors have reported a higher prevalence of CUA among infertile women [4,6]. However, Jayaprakasan et al. [14] found that although women with CUA represented 13.3% of their study population, the prevalence of major anomalies was 1.4%. As noted, only major anomalies were considered in our study.
Baseline characteristics were similar between the study and control groups, which strengthens our conclusions. However, the CUA group had a significantly longer duration of infertility. This may reflect greater difficulty in achieving a successful pregnancy, potentially due to implantation failure or early pregnancy loss [3,4,14]. Delayed referral for infertility assessment is another possible explanation, as diagnosis of CUA requires specialized imaging techniques that may not be routinely performed [15,16]. Considering the potential negative effect of CUA on fertility, a higher proportion of idiopathic infertility in the CUA group might have been expected, but this was not observed. Male and female factors (including tubal factors, ovulatory dysfunction, endometriosis, and low ovarian reserve) were used to classify infertility. When no cause was identified after couple assessment, infertility was classified as idiopathic in both groups. These findings highlight the uncertainty regarding the contribution of CUA to infertility.
The pregnancy rate after ART was similar in infertile women with CUA (classes U2, U3, and U4) and those with a normal uterus, consistent with a recent meta-analysis [8]. In that study, no significant difference in pregnancy rate was observed when all CUA classes were compared with controls (OR 0.87; 95% CI 0.7–1.08; p = 0.2; I2 = 70%) [8]. However, lower pregnancy rates were reported when classes were analyzed separately, including septate uterus and hemi-uterus, but not bicornuate uterus [8]. In our study, the smaller number of CUA cases limited analysis and comparison of outcomes across individual CUA classes.
Our study found no significant association between CUA and obstetric complications, including first-trimester pregnancy loss, preterm delivery, FGR, LBW, and cesarean delivery, which contrasts with findings from several previous studies. Venetis et al. [5] reported a higher risk of first-trimester miscarriage and preterm delivery in women with CUA. Kim et al. [8] confirmed these findings and additionally identified an increased risk of FGR and cesarean delivery. Other authors have reported conflicting results, with some identifying significant associations between CUA and adverse obstetric outcomes, and others finding no differences [11,14,17,18].
The discrepancy with previous studies may be explained by optimized hormonal stimulation and endometrial preparation in our cohort, which could have improved implantation and pregnancy rates [11,14], as well as by the heterogeneity in type and severity of CUA, particularly the predominance of milder anomalies such as partial septate uterus [6].
Regarding septoplasty, women with a complete septate uterus appeared to benefit from surgery, whereas those with a partial septate uterus had lower live birth rates. This observation should be interpreted with caution because of the very small sample size. Proposed pathogenetic mechanisms for poorer outcomes in septate uterus include inadequate uterine vascularization, uncoordinated contractions, altered composition of the fibroelastic connective tissue of the septum, and irregular hormonal responsiveness of the septal endometrium [19]. However, the influence of septum size remains unclear [19]. Rikken et al. [20] conducted a randomized controlled trial and concluded that septum resection did not improve outcomes compared with expectant management. Similarly, ESHRE guidelines state that evidence is insufficient to recommend routine septum resection [21]. Therefore, the effectiveness of hysteroscopic septoplasty remains controversial, as does the optimal surgical technique (electrosurgery versus mechanical) [22]. Nevertheless, in their systematic review, Fedele et al. [3] reported a reduced miscarriage rate after surgery in both partial and complete septate uterus.
Although this study provides relevant information on ART outcomes in women with CUA, it has an important limitation, namely the small number of cases with CUA diagnosis. In addition, diagnostic ultrasound examinations were performed by more than 10 sonographers who, although mostly adhering to ESHRE/ESGE guidelines, may have used different criteria for CUA diagnosis. Further multicenter studies are needed to clarify the impact of CUA subclasses on fertility and the effect of septum surgery.
In conclusion, pregnancy and live birth rates after ART were not significantly different between women with CUA and those with a normal uterus. No differences were observed in other ART outcomes. However, because of the small number of CUA cases, outcomes could not be compared across individual CUA classes and the normal uterus.
Contributors
Ana Luisa Arteiro and Ana Filipa Ferreira contributed to study conception and design, data collection, statistical analysis, and text preparation. All other authors contributed to text revision and approval of the final version to be published.
Data availability
The data that support our finding are available from the corresponding author (Ana Filipa Ferreira) upon reasonable request.