Introduction
Tubo-ovarian abscess (TOA) is a severe complication of pelvic inflammatory disease (PID), characterized by pus-filled collections involving the fallopian tubes and/or ovaries. The condition usually results from ascending genital tract infections or, less commonly, secondary spread from intra-abdominal sepsis. Approximately 30–40% of cases are polymicrobial, with common pathogens including Chlamydia trachomatis, Neisseria gonorrhoeae, Escherichia coli, anaerobes, and Actinomyces species in association with intrauterine devices (IUDs) [1]. Risk factors include IUD use, multiple sexual partners, early sexual debut, diabetes mellitus, HIV infection, and other immunocompromised states. However, TOA may also occur in women without identifiable risk factors [2].
Diagnosis relies on a combination of clinical features (fever, abdominal pain, adnexal tenderness, and purulent vaginal discharge), laboratory findings (elevated inflammatory markers and leukocytosis), and imaging (ultrasound, computed tomography [CT], or magnetic resonance imaging [MRI]). Although intravenous antibiotics remain the first-line treatment, up to 30–40% of cases require surgical or image-guided drainage [3]. We present a case series of three women with TOA, highlighting their varied clinical presentations, microbiological findings, and the need for surgical and multidisciplinary management.
Case presentations
Case 1
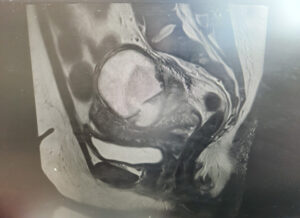
A 48-year-old woman presented with abdominal pain, fever (40.3 °C), nausea, and vomiting three days after undergoing hysteroscopic transcervical resection of a submucosal fibroid. Laboratory investigations showed a white cell count of 16.2 × 10⁹/L, neutrophils 13.9 × 10⁹/L, hemoglobin 102 g/L, and C-reactive protein 83 mg/L. She was started on intravenous co-amoxiclav and amikacin.
CT imaging demonstrated right hydrosalpinx with bilateral ovarian cysts (Figure 1), while MRI confirmed bilateral tubo-ovarian complexes (Figure 2). She underwent laparoscopic drainage of the abscess, adhesiolysis, and pelvic washout, with an estimated blood loss of 800 mL. Blood cultures grew ESBL-producing Escherichia coli, and antibiotics were escalated to intravenous meropenem. She was discharged after eight days on oral ciprofloxacin and metronidazole to complete a 10-day course.
Case 2
A 32-year-old para 4 woman presented with severe abdominal pain. Laboratory results showed hemoglobin 71 g/L, white cell count 15.4 × 10⁹/L, and C-reactive protein 236 mg/L. She received intravenous co-amoxiclav and metronidazole, along with oral doxycycline.
CT imaging revealed a complex cystic lesion in the pouch of Douglas with involvement of the left ureter and hydroureteronephrosis (Figure 3). MRI confirmed a left TOA with associated iliopsoas myositis and posterior cervical wall invasion (Figure 4). Ultrasound-guided drainage was attempted but was unsuccessful because of adjacent bowel loops. A ureteric stent was inserted, followed by laparoscopic drainage of the abscess (500 mL of pus) and right cystectomy with adhesiolysis. She was tested for tuberculosis and HIV, both of which were negative. She recovered well and was discharged four days postoperatively, with planned ureteric stent removal at follow-up.
Case 3
A 44-year-old woman presented with severe abdominal pain, fever, dysuria, and offensive vaginal discharge. Examination revealed right iliac fossa tenderness with guarding and rebound. Laboratory tests showed a white cell of 10.2 × 10⁹/L and C-reactive protein 232 mg/L. CT imaging demonstrated an inflammatory mass in the right hemipelvis consistent with a TOA (Figure 5). She underwent exploratory laparoscopy with adhesiolysis, pelvic washout, salpingo-oophorectomy, and JJ stent insertion. Pus culture grew Streptococcus constellatus. Despite initial improvement, she developed worsening sepsis three days postoperatively. Repeat CT revealed a large pelvic collection and bilateral pleural effusions. She subsequently underwent ultrasound-guided drainage, with clinical resolution.
Discussion
Tubo-ovarian abscess (TOA) represents one of the most severe complications of PID, with a clinical course that ranges from localized pelvic infection to life-threatening systemic sepsis. TOA is typically associated with ascending infection from the lower genital tract, although gastrointestinal sources have also been reported. Risk factors include PID, IUD use, recent uterine instrumentation or gynecologic procedures, multiple sexual partners, diabetes mellitus, and immunocompromised states. Despite these recognized risk factors, TOA can develop in women without any of them, as illustrated by post-procedural cases following minimally invasive gynecological interventions.
The clinical presentation of TOA is often nonspecific, contributing to diagnostic delays. Most patients experience lower abdominal or pelvic pain, while a smaller proportion present with vaginal discharge or bleeding. Approximately half exhibit systemic features such as fever, nausea, and vomiting. On physical examination, findings are frequently limited, with variable degrees of pelvic tenderness or adnexal fullness. Laboratory investigations typically reveal leukocytosis and elevated inflammatory markers, though these findings lack specificity [2,4].
Diagnostic imaging plays a central role in the evaluation of suspected TOA. Transvaginal and transabdominal ultrasonography are preferred as the initial modalities for assessing pelvic pain in reproductive-aged women. When ultrasonographic findings are inconclusive, CT or MRI may be performed for further evaluation. CT offers higher sensitivity and can help distinguish TOA from gastrointestinal pathologies with similar presentations. Typical CT features include a complex, solid-cystic adnexal mass with thick, irregular, enhancing walls and septated internal fluid. Additional findings may include thickening of the mesosalpinx, dilated fallopian tubes, periovarian fat stranding, and reactive inflammatory changes such as peritoneal fluid, bowel wall thickening, hydronephrosis, or ileus. MRI is particularly valuable when further differentiation is required, as it provides superior soft-tissue contrast and detailed visualization of tubal structures. Characteristic MRI features include thick-rim and septal enhancement after intravenous gadolinium administration and restricted diffusion of purulent content on diffusion-weighted imaging [2].
The three cases presented illustrate the clinical and radiological diversity of TOA and its potential complications. The first case highlights the risk of post-procedural TOA following hysteroscopic fibroid resection. Although minimally invasive gynecological procedures are generally safe, they may predispose to ascending infection, particularly in the presence of subclinical PID. This observation supports previous literature indicating that TOA can occur in women without conventional risk factors such as IUD use or multiple sexual partners [2]. The second case demonstrates the potential for rare but serious extra-pelvic spread, with iliopsoas myositis and ureteric obstruction secondary to TOA. Such complications, while uncommon, underscore the importance of early imaging and multidisciplinary involvement—including radiology, urology, and infectious disease specialists—to optimize management. Similar to recent reports of pelvic abscesses extending beyond the adnexa [3]. The third case highlights the challenge of persistent infection despite surgical intervention, necessitating subsequent image-guided drainage. This reflects the complementary role of interventional radiology in managing refractory pelvic collections [1,5].
The microbiological profile of TOA is typically polymicrobial, reflecting both vaginal and enteric flora. Commonly isolated organisms include Escherichia coli and anaerobic bacteria such as Bacteroides species. Notably, Streptococcus constellatus was identified in the third case, emphasizing the diversity of potential pathogens and the importance of initiating broad-spectrum empirical antibiotics until culture results are available.
Management of TOA requires a stepwise, individualized approach. Broad-spectrum intravenous antibiotics remain the cornerstone of initial therapy. However, failure of medical management—more likely in patients with bilateral abscesses, large collections, or advanced age—necessitates escalation to surgical or radiological intervention. Surgical drainage and image-guided percutaneous aspiration are both effective in controlling infection and preventing complications. This escalation pathway—antibiotics followed by surgery or image-guided drainage when required—represents best practice and has been associated with improved outcomes.
Early recognition of TOA is critical, as delayed diagnosis increases the risk of rupture, sepsis, and long-term sequelae such as tubal-factor infertility, ectopic pregnancy, and chronic pelvic pain. Multidisciplinary collaboration across gynecology, radiology, and infectious diseases is essential to achieving favorable outcomes, particularly when complications extend beyond the pelvis. Ultimately, individualized, escalation-based management provides the best balance between infection control and fertility preservation [6].
Conclusion
TOA is a complex gynecological emergency with variable clinical presentations. Antibiotics alone are often insufficient, and escalation to surgical or radiologic drainage may be required. These cases highlight the importance of early recognition, individualized care, and multidisciplinary collaboration in managing TOA and preventing long-term complications.