Introduction
Congenital uterine anomalies arise from maldevelopment of the Müllerian ducts during intrauterine life [1]. They affect approximately 5.5% of the general population, with significantly higher prevalence among individuals with infertility and/or recurrent early pregnancy loss; in fact, up to 25% of patients with both conditions may be affected [1,2]. Some patients remain completely asymptomatic, leading to incidental diagnosis during routine pregnancy ultrasound or even at delivery. Others may present with cyclic pelvic pain, dysmenorrhea, or adverse reproductive outcomes such as recurrent miscarriage, infertility, preterm birth, fetal malpresentation, fetal growth restriction, placental abruption, or stillbirth, prompting further evaluation and diagnosis through appropriate imaging. Three-dimensional ultrasound and Magnetic Resonance Imaging (MRI) are recognized as standard diagnostic tools for Müllerian anomalies [1,3].
Multiple classification systems exist, with substantial variations across medical societies. The most widely used are those proposed by the American Society for Reproductive Medicine (ASRM) and the joint system developed by the European Society of Human Reproduction and Embryology and the European Society for Gynaecological Endoscopy (ESHRE/ESGE), both intended to standardize terminology, facilitate research, and improve diagnostic and clinical management [²,4,5]. Each system can accurately describe the clinical case presented here.
Uterine rupture is a rare but severe obstetric emergency associated with significant maternal and neonatal morbidity and mortality. Recognized risk factors include prior uterine surgery—such as cesarean delivery or myomectomy—as well as congenital uterine anomalies, abnormal placentation, and multiple gestation, among others [6,7]. Spontaneous uterine rupture in a non-laboring patient is exceedingly uncommon and may carry catastrophic consequences for both mother and fetus [⁶]. In this paper, we present a case of second-trimester uterine rupture with fetal demise in a woman with a previously undiagnosed Müllerian anomaly. This rare presentation underscores the importance of early pregnancy ultrasound to identify conditions that warrant specialized obstetric surveillance and management.
Case report
A woman in her twenties, gravida 1 para 0 at 21 weeks’ gestation, with no relevant medical or surgical history, presented to the Emergency Room with pelvic pain. She had attended all scheduled prenatal visits without notable findings. A first-trimester abdominal ultrasound, performed at 12 weeks and 3 days at an outside facility, was reviewed; the report contained no remarks regarding the uterus or adnexa, and no images were available for reassessment.
For two weeks prior to diagnosis, she had been experiencing intermittent, colicky right-sided abdominal pain without gastrointestinal or urinary symptoms. During a previous Emergency Department visit, abdominal tenderness was noted, but the patient left against medical advice before further evaluation could be completed. Three days later, she returned with worsening abdominal pain. On examination, she was hypotensive, her abdomen was distended, and she exhibited clear signs of peritoneal irritation. Fluid resuscitation was initiated, and an abdominal ultrasound revealed a live fetus and a moderate amount of free intraperitoneal fluid. Shortly thereafter, the patient collapsed under observation, prompting an emergency exploratory laparotomy.
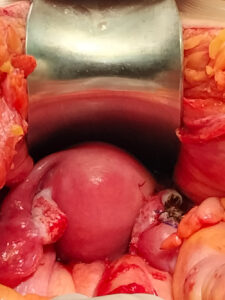
During surgery, approximately 1.5 liters of blood were aspirated from the abdominal cavity. A non-viable fetus was found free-floating in the peritoneal cavity, and a previously unrecognized uterine anatomical anomaly was identified: a ruptured right-sided rudimentary horn connected to a left unicornuate uterine cavity by a two-centimeter fibrous band, which continued into a normally developed cervix. Each uterine horn was associated with its ipsilateral fallopian tube and ovary, as shown in Figures 1 and 2.
The observed anatomy was consistent with a Class U4aC0V0 uterine malformation according to ESHRE/ESGE classification criteria—a hemi-uterus with a functional, communicating rudimentary horn and a single cervix and vaginal canal [²]. According to ASRM criteria, it corresponded to a unicornuate uterus with an associated right uterine remnant containing functional endometrium [⁴].
The ruptured rudimentary horn and the ipsilateral fallopian tube were excised without complication, and the unicornuate uterus was preserved, as shown in Figure 2. Postoperatively, the patient achieved hemodynamic stability in the Intensive Care Unit, requiring a total of six units of red blood cells. Her subsequent recovery was uneventful, and she was discharged after seven days of hospitalization. Histopathology confirmed a rudimentary uterine cavity and a 21-week pregnancy.
Subsequent clinical and imaging evaluations were performed to exclude associated congenital anomalies, including renal tract abnormalities. MRI confirmed a unicornuate uterus, two normally developed ovaries, and a single cervix and vagina. Six months after surgery, hysteroscopy revealed a distensible uterine cavity with a unilateral tubal ostium and preserved endometrial architecture, with no additional anatomical variants identified. The patient resumed regular menstrual cycles within three months of surgery and continues follow-up for reproductive planning. She has been counselled regarding the potential reproductive risks associated with a unicornuate uterus.
Discussion
Müllerian congenital anomalies can significantly affect quality of life, fertility, and pregnancy outcomes. This case illustrates a spontaneous second-trimester uterine rupture in a patient with a previously undiagnosed uterine anomaly—an uncommon but potentially catastrophic presentation.
Three-dimensional transvaginal ultrasound is a safe, non-invasive, and widely accepted diagnostic tool for Müllerian anomalies; however, its utility as a universal screening method remains limited due to availability and cost considerations. In addition, routine ultrasound for preventive care is not recommended by major professional societies, including the American College of Obstetricians and Gynecologists (ACOG) [8], the Royal College of Obstetricians and Gynaecologists (RCOG) [1], and the Centers for Disease Control and Prevention (CDC) [9]. Despite these limitations, timely and accurate diagnosis—ideally in the preconception period or early antenatal care—may prevent life-threatening complications and improve counselling regarding potential adverse reproductive outcomes [10,11].
According to the Practice Guidelines of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) [12], first-trimester ultrasound should include confirmation of intrauterine pregnancy location using a sweep encompassing the entire uterus. Such systematic assessment allows early diagnosis of extra uterine pregnancies, cesarean scars pregnancies and uterine malformations and prompt proper management of these conditions. We believe that in our case earlier diagnosis could have prevented such an emergent presentation and prompt earlier intervention.
Diagnosing uterine rupture in an otherwise healthy second-trimester pregnant woman with no identifiable risk factors can be challenging [14]. More common causes of abdominal pain—such as appendicitis, ruptured ovarian cyst, or ovarian torsion—are typically considered first. In this case, the patient’s hemodynamic instability prompted an emergency laparotomy, which immediately confirmed the diagnosis of uterine rupture and enabled timely, life-saving management. This underscores the need to keep rare but time-sensitive conditions such as spontaneous uterine rupture within the differential diagnosis.
Bhagavat’s paper reviews surgical management options for a unicornuate uterus with either a functional or non-functional rudimentary horn, ranging from straightforward horn excision to more complex procedures aimed at reconstructing a normal uterine cavity. The authors conclude that additional studies are required to establish clearer guidance for managing these anomalies [13].
A review of the literature identified a similar Müllerian anomaly described in a case report in which the diagnosis was made incidentally during a third uneventful cesarean section. All three pregnancies progressed to term, as implantation occurred in the unicornuate uterus rather than in the rudimentary horn—accounting for the markedly different obstetric outcomes compared with our case [15].
In conclusion, this case underscores the importance of recognizing the true prevalence of Müllerian anomalies and the potential impact that early diagnosis—particularly during the first trimester—can have on maternal and neonatal outcomes. As recommended by ISUOG [12], first-trimester ultrasound should include a thorough evaluation of the uterus and adnexa to identify anatomical variants that may necessitate tailored pregnancy surveillance. It is also essential to consider rare but life-threatening conditions such as spontaneous uterine rupture in the differential diagnosis, as timely recognition is crucial for initiating life-saving interventions. With appropriate surgical management and follow-up, we believe our patient can anticipate a successful reproductive future despite the obstetric challenges associated with a unicornuate uterus.
Disclosures
Author contribution
Beatriz Maria Neves, Alexandra Pregal, Diana Conceição Arteiro contributed to patient care, conception of the case report, acquiring and interpreting the data, undertaking the literature review and critically revising the article for important intellectual content.
Cláudio Rebelo, Mariana Valente Abreu contributed critically revising the article for important intellectual content as well as to the initial diagnosis of the pathology, collaborated in the interpretation, and assisted in the writing of the manuscript.
Beatriz Maria Neves, Alexandra Pregal, Diana Conceição Arteiro contributed to the care and follow-up of the patient.
All authors approved the final submitted manuscript.
Patient consent and ethics
Patient consent was obtained for the publication of this case report.
Ethical considerations were upheld throughout the evaluation of this case, publication that was authorized by the institution’s research and ethics committee. Measures were taken to ensure the confidentiality of information and patient anonymity.
Abbreviations
- ACOG - American College of Obstetricians and Gynecologists
- ASRM - American Society of Reproductive Medicine
- CDC - Center for Disease Control and Prevention
- ESHRE/ESGE - European Society for Human Reproduction and Embryology and European Society of Gynaecological Endoscopy
- ISUOG - International Society of Ultrasound in Obstetrics and Gynecology
- MRI - Magnetic Resonance Imaging
- RCOG - Royal College of Obstetricians and Gynecologists