Introduction
growth and a high tendency to recur after surgical resection [1]. Although it does not metastasize and its histology appears benign, the tumour commonly infiltrates soft tissues of the pelviperineal region, making surgical excision difficult. Incomplete resection, or resection without free margins, substantially increases the risk of recurrence, and infiltration of adjacent organs may have functional consequences if a radical approach is attempted [2–3]. As a result, management is often complex, and high-quality evidence to guide decision-making remains limited.
First described in 1983, and with approximately 250 published cases in various anatomical locations [4], aggressive angiomyxoma is classified as a mesenchymal tumour with a myxoid stroma, abundant vasculature, and spindle-shaped cells [5]. It most frequently arises in the pelvic and perineal regions, involving structures such as the vulva, vagina, perineum, rectum, and occasionally the presacral space [2]. Angiomyxomas are broadly divided into superficial and aggressive subtypes. The superficial type is more localized and less infiltrative, occurring mainly in the dermis or subcutaneous tissues. In contrast, the deep aggressive variant, as in the present case, shows extensive infiltration within the pelvic and perineal compartments.
The tumour affects women predominantly in their reproductive years, supporting a possible hormonal influence on its development and growth. Despite its benign classification, it infiltrates surrounding tissues without respecting anatomical boundaries and often recurs even after apparently wide resections [6]. The preferred treatment is surgical excision with tumour-free margins [7]. However, achieving negative margins is frequently challenging because of its deep location and proximity to critical structures such as the rectum, bladder, pelvic floor, and reproductive organs. Attempting extensive resection may compromise organ function or lead to significant morbidity. Moreover, unlike many solid tumours, aggressive angiomyxoma shows poor response to radiotherapy and chemotherapy, limiting options when residual or recurrent disease is present [8].
Recent studies have demonstrated expression of estrogen and progesterone receptors in many angiomyxomas [9]. This has supported the use of hormonal therapy—primarily gonadotropin-releasing hormone (GnRH) analogues and aromatase inhibitors—as adjuvant treatment, particularly in premenopausal women, aiming to suppress potential hormone-driven tumour stimulation.
The following case describes an aggressive pelvic angiomyxoma diagnosed in a middle-aged woman and managed with surgery followed by adjuvant hormonal therapy. It highlights diagnostic and therapeutic challenges, the importance of long-term surveillance, and the current limitations of management strategies, which remain based more on biological rationale than on robust scientific evidence [13–14].
Case report
The patient was a 44-year-old woman who presented with a progressively enlarging mass in the external genital area. She had first noticed it 4 months earlier, with gradual growth but no bleeding, significant pain, dyspareunia, or urinary or bowel changes. She reported only a sense of heaviness and mild local discomfort.
Her medical history was unremarkable. She had no prior pelvic surgeries other than two eutocic deliveries, the last in 2012, with episiotomy. She had used combined oral contraceptives for ten years, discontinued after being diagnosed with severe factor XII deficiency, although she remained asymptomatic. Family history included maternal endometrial cancer at age 65; her mother died at 70 from stroke.
On physical examination, a soft, non-tender mass was palpated extending from the right posterior vaginal wall toward the right ischiorectal fossa. It measured approximately 5–6 cm and lay partly beneath the previous episiotomy scar. The overlying mucosa and skin were intact. Because of its location and consistency, a provisional diagnosis of levator ani muscle avulsion had been considered by her private gynecologist, prompting referral.
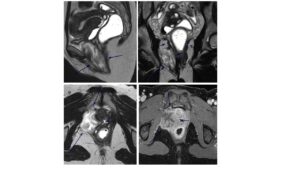
To evaluate pelvic floor integrity and better characterize the lesion’s location, size, and anatomical relationships, MRI with dynamic defecography was requested, partly at the patient’s insistence based on prior advice. MRI showed a well-defined mass measuring 8 × 3 × 4 cm between the anterior rectal wall and the right posterior-inferior vaginal wall, extending into the vulvar region and infiltrating the puborectalis muscle. No nodes or distant disease were identified. The lesion was hyperintense on T2-weighted images with linear hypointense “swirling” areas, consistent with a myxoid matrix. There was no fat suppression on T2 fat-sat sequences. DWI showed high signal without restriction. Post-contrast images demonstrated intense enhancement of fibrous components. The radiologist considered these features highly suggestive of aggressive angiomyxoma (Figure 1), given the myxoid signal, vascular voids, and characteristic pattern of dissecting through pelvic compartments.
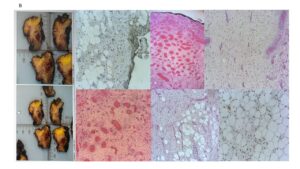
A core needle biopsy confirmed the diagnosis. Histology showed spindle-cell proliferation within a myxoid stroma and abundant vasculature, without atypia or mitotic activity (Figure 2). Immunohistochemistry showed estrogen and progesterone receptor expression, supporting hormonal sensitivity.
The case was discussed at the multidisciplinary tumor board, which recommended surgical resection despite acknowledging that complete tumor-free margins were unlikely due to proximity to the rectum and levator ani musculature. Preoperative hormonal blockade with gonadotropin-releasing hormone (GnRH) analogues plus an aromatase inhibitor was initiated to suppress hormonal stimulation until surgery.
Surgical removal of the mass was performed, aiming for macroscopically clear margins while prioritizing preservation of adjacent organs. No intra- or postoperative complications occurred. Pathology confirmed the diagnosis and reported involved margins, indicating microscopic residual tumor.
Given the positive margins, postoperative treatment with continued ovarian suppression using GnRH analogues together with an aromatase inhibitor was maintained. Follow-up included clinical evaluation and serial MRI. A baseline MRI was performed shortly after surgery, followed by scans every six months. At 2.5 years of surveillance, no evidence of recurrence had been detected. The patient remained asymptomatic, with no signs of pelvic compression or new masses on physical examination or transvaginal ultrasound.
Targeted hormonal therapy was well tolerated. She reported mild menopausal symptoms—hot flushes, light insomnia, and amenorrhea—which were managed conservatively. The patient provided informed consent for publication of this case.
Discussion
Aggressive angiomyxoma poses notable diagnostic and therapeutic challenges. Although histologically benign, its clinical behavior resembles that of a locally infiltrative malignancy, with a marked tendency for local recurrence—hence the term “aggressive.” Because of its rarity and nonspecific presentation, it is frequently misdiagnosed as more common perineal or pelvic lesions such as Bartholin cysts, lipomas, perineal hernias, pelvic floor tumours, or pseudomyxomas, as occurred in our patient. This highlights the importance of a thorough clinical evaluation supported by appropriate imaging, with MRI being the most informative modality for assessing extension, tissue planes, and surgical planning.
Histopathologically, the tumour shows a myxoid matrix with sparse spindle cells and abundant vasculature, typically without atypia or mitosis. This benign microscopic appearance can be misleading; the infiltrative growth pattern is what makes the tumour difficult to manage. Complete surgical resection with negative margins remains the cornerstone of treatment. Successful removal of lesions up to 12 cm with no recurrence has been documented [8]. However, complete excision is often unachievable without risking injury to adjacent organs such as the rectum, bladder, or reproductive structures [15]. When margins are compromised, recurrence risk increases, making it necessary to balance oncologic completeness with preservation of organ function. Multidisciplinary evaluation is therefore essential, especially when potential postoperative sequelae must be weighed against the likelihood of recurrence [16].
Chemotherapy and radiotherapy have limited roles in this tumour because of its low proliferative index, which confers resistance to cytotoxic modalities [8]. In contrast, hormone receptor positivity—reported in up to 90% of cases—provides a biological rationale for hormonal therapy, especially when surgery is incomplete or recurrence risk is high [15]. Evidence, although limited, suggests that GnRH analogues and aromatase inhibitors may reduce tumour volume preoperatively and help prevent recurrence postoperatively (Table 1). Combined suppression in premenopausal women induces profound hypoestrogenism, theoretically reducing tumour stimulation.
Case series published between 2012 and 2020 report favorable outcomes with GnRH analogues in receptor-positive tumours, with fewer recurrences observed among treated patients [17]. Rare presentations during pregnancy have also been described, including one in a twin gestation successfully managed surgically with good maternal and fetal outcomes [18]. Such scenarios reinforce the need for individualized therapeutic strategies and close coordination between specialties.
In our patient, the presence of infiltrative disease and positive margins placed her at high risk for recurrence. Hormonal therapy was therefore advised and accepted. While it is impossible to know the natural course had she not received adjuvant treatment, it is reassuring that she remains disease-free to date. This case contributes to the limited but growing literature on optimal management of aggressive angiomyxoma and underscores the importance of clinical suspicion, appropriate imaging, multidisciplinary planning, and long-term follow-up.
Conclusion
A combined approach of conservative surgery and hormonal suppression has, in this case, achieved short- and medium-term disease control. Nonetheless, long-term vigilance is essential, as aggressive angiomyxoma may recur many years after initial treatment. Surveillance should therefore be structured, ideally with periodic MRI, given that recurrences are frequently asymptomatic.
Management must be individualized, considering tumour extension, anatomical location, patient age, potential functional consequences of extensive surgery, hormonal receptor status, and feasibility of prolonged follow-up. Although evidence for hormonal therapy and its optimal duration remains limited, its biological plausibility makes it a reasonable adjuvant option—particularly when margins are positive or complete excision is not feasible.
Disclosures
Author contributions
L. Villaescusa: Conceptualization, Investigation, Visualization, Writing original draft, Writing review & editing; S. López-Celada: Visualization, Writing review & editing; J. Utrilla: Investigation; V. Aranaz: Visualization; J. Onrubia: Visualization, Writing review & editing; F. Quereda: Conceptualization, Investigation, Writing review & editing, Supervision.
Statement of ethics
Patient provided signed informed consent for the publication of her case.