Climate change triggers a health crisis that increases the burden on healthcare systems, societies, and economies and has been declared the single biggest health threat facing humanity by the World Health Organization (WHO) [1]. Increased temperatures, air pollution, environmental toxins, and extreme weather events result in negative health outcomes such as non-communicable, vector-borne, and waterborne diseases, malnutrition, mental health conditions, heat-related illness, and mortality [1,2].
By exacerbating existing gender-related health inequities, climate change disproportionately impacts the morbidity and mortality of women compared to men. This is particularly evident for women in low-to-middle income countries (LMICs) due to socioeconomic, cultural, and structural factors that limit their adaptive capacity and access to care [2-5].
This narrative review focuses on the disproportionate impact of climate change on women’s health and outlines clinical, educational, and community-level strategies and practical interventions that healthcare professionals (HCPs) and healthcare workers (HCWs) can implement. The aim is to help women manage the effects of climate change and empower them to take action to reduce health inequities and mitigate their risk of harm.
The impacts of climate change on women’s health outcomes across the lifespan
Climate change impacts women’s health in different ways across the lifespan (Figure 1), including during puberty, sexual maturation, pregnancy, lactation, perimenopause, and menopause. Individual risks are often compounded by factors such as age, ethnicity, marital status, disabilities, employment, education, caregiving responsibilities, and psychosocial well-being [6-11]. Approaching climate-related threats from a holistic, life course perspective is essential for understanding the specific risks and vulnerabilities faced by women at different life stages, thereby identifying opportunities for targeted interventions.
Socioeconomic inequities exacerbate women’s physiological vulnerabilities by increasing their exposure to risks while limiting adaptive capacity. Globally, women make up 70% of those living below the poverty line in LMICs [12,13]. In these countries, women’s greater physiological susceptibility to adverse effects of heat stress and pollution is compounded by a lack of access to cooling or fresh water, as well as increased exposure to indoor air pollution from cooking gases [14]. In the event of drought or flooding, women are often disadvantaged when confronting the challenges posed by displacement, resource scarcity, poor agricultural working conditions, loss of income and livelihoods, disruption of healthcare services, and increased risk of sexual- and gender-based violence (SGBV) [15,16]. LMICs are also most frequently hit by climate disasters, with regions such as parts of Southeast Asia, Northern South America, and Central Africa projected to experience the highest impact from floods by 2050 [14].
To safeguard women’s health and improve outcomes, it is essential to adopt adaptive strategies that anticipate, prepare for, and mitigate the health impacts of climate change in routine care, public and community health initiatives, and emergency responses following extreme weather events [14].
Physiological susceptibilities and the importance of health literacy
Sex-based differences in thermoregulation contribute to higher heat-related mortality among women during extreme heat events, with some studies reporting rates up to twice those observed in men [2]. Inhaled particulate pollutants also appear to deposit more extensively in female pulmonary systems, potentially increasing their susceptibility to non-communicable diseases (NCDs), particularly those affecting the cardiovascular and respiratory systems [17].
Health literacy plays a central role in enabling women to interpret and act on public health guidance. Improving women’s awareness of climate-sensitive health conditions may support adaptive behaviors, especially during physiologically vulnerable periods such as pregnancy and lactation [18,19]. Educational materials should be designed with input from local women to ensure cultural and contextual relevance, which may in turn improve uptake [20]. Where feasible, collaborative design approaches should be adopted to align content with community norms and information needs [21]. Furthermore, messaging should be tailored to local contexts and delivered through appropriate channels, whether interpersonal communication, printed materials, digital platforms, or community events. Ideal dissemination points may include primary care clinics, hospitals, schools, and public or corporate spaces that experience high traffic.
In many rural and underserved settings, primary care providers represent the only consistent point of contact with healthcare. They therefore play a crucial role in identifying early signs of climate-related health risks, providing anticipatory guidance, and facilitating access to care. Integrating climate risk assessments into routine consultations, particularly for pregnant women, older adults, and those with chronic conditions, could enhance early intervention. Community leaders may also serve as effective intermediaries in communicating climate-health information and promoting both individual and collective mitigation strategies.
Psychosocial impacts and sexual- and gender-based violence in climate-affected settings
Beyond the immediate physical risks posed by extreme weather events, environmental disasters such as floods, droughts, and hurricanes often exacerbate existing gender inequities and contribute to mental health disorders [22]. Elevated rates of depression, anxiety, and post-traumatic stress disorder have been documented in affected populations, particularly among women in caregiving roles or from socioeconomically disadvantaged or rural communities. These outcomes are frequently compounded by limited access to mental health services and persistent stigma surrounding psychological distress.
In addition, climate-related disasters are associated with an increased incidence of SGBV, including intimate partner violence, trafficking, and child marriage. These risks are heightened in contexts of infrastructure collapse, displacement, and economic instability, where protective systems are weakened or absent [21,23].
As often the first responders in environmental crises, HCPs and HCWs have a critical role to provide the minimum initial service package of food, shelter, water, and social protections that is inclusive of sexual and reproductive health (SRH) services while identifying and supporting women affected by trauma and SGBV. Integrating gender-sensitive screening for mental health conditions and SGBV into routine care, alongside efforts to create safe, confidential environments for disclosure, can facilitate timely intervention, as can improved inter-agency coordination, better inclusion/engagement of local initiatives and civil societies in SRH services delivery, improved quality of SRH services, adequate and regular training of healthcare providers, and increased awareness among women and girls [24,25]. These measures should be supported by access to culturally appropriate psychosocial and reproductive health services.
Reproductive health vulnerabilities and the role of contraceptive access
Climate change has been associated with the exacerbation of various reproductive health conditions, including endometriosis, fibroids, polycystic ovarian syndrome, and early menopause. While these conditions can affect all individuals with female reproductive systems, structural inequities in access to care, education, and resources often intensify their impact on women, particularly in low-resource settings [6,7,26-28].
Efforts to reduce unplanned pregnancies can yield indirect benefits for women’s health by mitigating maternal exposure to climate-related risks and alleviating pressure on strained health and environmental systems [7,19,29-33]. Increasing access to contraception thus represents an intervention with multiple downstream benefits, including reductions in maternal morbidity, unsafe abortion, and pregnancy complications [34].
Hormonal contraceptives reduce menstrual bleeding for many women and, in some cases, induce amenorrhea. These effects may be advantageous in environmental settings where management of menstrual pain and bleeding and sourcing personal hygiene products can present additional stressors for women already facing resource scarcity, displacement, lack of privacy, and elevated risks of SGBV and post-traumatic stress [19]. In particular, hormonal intrauterine devices offer a reliable, value-for-money option in resource-constrained settings, as their efficacy is not dependent on daily adherence or continuous supply chains.
Climate-related risks during pregnancy and early life
Pregnancy is a period of heightened physiological vulnerability, during which climate-related factors can adversely impact both maternal and fetal health. Air pollution and extreme heat are associated with complications such as miscarriage, preterm birth, low birth weight, stillbirth, gestational diabetes, hypertensive disorders of pregnancy, and congenital abnormalities [7,19,29-33].
Evidence has linked maternal exposure to environmental pollutants with altered immune function, endocrine disruption, neurodevelopmental delay, and susceptibility to NCDs and neuropsychiatric disorders in later life [7,35-37]. Climate-driven expansion of mosquito habitats following flooding compounds these risks, transmitting infections from cholera and dysentery to others such as malaria, dengue fever, and Zika virus, which can lead to complications including fetal growth restriction, preterm birth, congenital abnormalities, and maternal morbidity and mortality [19,38-42]. Pregnant women and children affected by waterborne diarrheal diseases, such as cholera, typhoid, and dysentery, are at particular risk of morbidity and mortality from these infections. All of these health threats can be further amplified during outbreaks of emerging infections such as Ebola and COVID, when access to primary healthcare services can become dramatically reduced [43,44].
Midwives and HCWs often serve as the first point of contact for pregnant women, particularly in low-resource or disaster-affected settings. Targeted training for these workers allow them to provide anticipatory guidance on climate-related risks, deliver psychosocial support, and adapt care delivery to environmental conditions [45]. Mobile clinics can help extend access to care in remote areas, while scheduling visits to avoid peak heat exposure can improve safety and uptake [20]. In urban areas, integrating air quality alerts into prenatal care apps or text messaging systems may help women reduce exposure on high-pollution days.
Expanding access to pre-, inter-, and post-conceptional counseling tailored to climate-related health risks could enhance the identification and management of modifiable risk factors before and after pregnancy. Optimizing maternal health through improved nutrition, lifestyle, medication management, and lifestyle interventions may reduce women’s susceptibility to heat stress, pollution, and other environmental hazards, thereby lowering the risk of adverse outcomes such as preeclampsia and preterm birth [46,47]. Furthermore, routine prenatal care during pregnancy offers an opportunity to monitor maternal and fetal health while educating women about climate-related risks and protective strategies. Postpartum, inter-conceptional counseling can also be used to address conditions that develop during pregnancy, reduce recurrence in future pregnancies, and support maternal health in the long term [46,47].
Health during midlife and menopause in a changing climate
The menopausal transition marks another period of increased vulnerability to climate-related stressors. Exposure to heat and pollution has been associated with elevated risks of cardiovascular disease and cognitive decline in postmenopausal women [6]. Nutritional deficiencies linked to food insecurity may further compromise bone health, aggravating the risks of osteoporosis and fracture in a population already susceptible due to declining estrogen levels [6]. Heat can also exacerbate vasomotor symptoms (hot flashes and night sweats) experienced by many women during the menopausal transition, which can negatively impact quality of life [6].
Despite these risks, targeted climate-health interventions for menopausal women remain limited [6]. HCPs and HCWs should consider individual risk profiles when caring for women in midlife, particularly in regions where extreme heat or high levels of pollution are commonplace [6]. Encouraging the adoption of cooling and hydration strategies, limiting pollution exposure, and monitoring cardiovascular, skeletal, and cognitive health may be beneficial [6].
Equipping the health workforce to address climate-driven women’s health challenges
Improving training and continuing education for HCPs and HCWs are essential to equip them with the knowledge needed to support women in managing the health impacts of climate change. This could include advising women on strategies to reduce climate-related health risks by offering practical guidance on hydration, heat avoidance, and awareness of medications that may interfere with the body’s homeostatic responses and impair thermoregulation [48].
Currently, there are limited climate-health resources tailored to general practitioners, obstetricians and gynecologists, nurses, midwives, and community HCWs. Educational materials that specifically address women’s health and climate change are also lacking. However, some foundational tools exist; in 2024, the WHO Academy and WHO Climate Change and Health Unit launched an interactive online training module aimed at building technical capacity to address context-specific health risks [49]. The WHO has also developed a toolkit to support HCPs and HCWs in engaging with patients on the health effects of climate change [50]. Nonetheless, these resources do not yet incorporate a gender-specific lens, and there is a need for materials that address women’s unique climate-related vulnerabilities.
HCPs and HCWs can help to develop and integrate climate- and women’s health-informed content into medical education curricula to improve knowledge and practice. A model similar to that employed by the European Network on Climate & Health Education, an initiative led by the University of Glasgow, could be adopted. This initiative aims to introduce lessons on climate change-related health challenges into the existing medical curricula, thus equipping students with the knowledge and skills needed to respond to the impacts of climate change on human health [51]. The network has brought together 38 medical schools across Europe, with an aim to train 10,000 students over the next three years through updating medical curricula, sharing best practices, and developing educational resources [51].
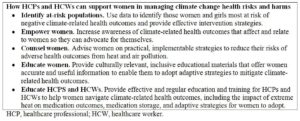
To ensure educational programs are contextually appropriate and widely accessible, local HCPs, HCWs, and community pharmacists should participate in the design and delivery of training. These providers, particularly in rural or underserved areas, may currently lack access to up-to-date information or formal training. Their involvement helps ensure interventions are culturally relevant, feasible to implement, and capable of reaching women in remote communities [52,53]. An overview of how HCPs and HCWs can support women to manage the risks of climate change on their health is shown in Table 1.
Challenges and barriers
Strengthening primary care and broadening healthcare infrastructure, embraced within a One Health framework, are essential for building resilience to climate-related threats [54]. At present, there is a lack of gender-disaggregated data and evidence-based interventions addressing the specific impacts of climate change on women’s health.
Robust data are therefore needed to provide the foundation for a clear evidence base. This can then guide clinical practice and policy-related decision-making aimed at managing the effects of climate change on women’s health within healthcare systems [18,21]. Dedicated investment is also necessary to support gender-focused climate-health initiatives, including those that consider the intersection of women’s health issues with SGBV and social vulnerabilities [55].
Conclusions
Women represent an underreported, understudied, and underprioritized group in the context of healthcare, and this inequity is exacerbated by climate change. As a group, women and those they care for, primarily children and elderly family members, are disproportionately impacted [19]. While some strategies exist to reduce these harms, more robust research is needed to inform health protection measures. Effective action in the form of rapidly implementable educational programs, clinical practice-based interventions, and community-based strategies is urgently required to manage the far-reaching impacts of climate change on women’s health. Effective action must include collaboration between legislative, policy, academic, and research sectors to prioritize addressing women’s health in a changing climate. Only by recognizing the interdependence of all sectors in effective change for women can a fundamental impact on women’s health today – and that of her future offspring and future generations – be achieved.