Acronyms and abbreviations
TVS: Transvaginal sonography; PPV: Positive predictive value; NPV: Negative predictive value; LR+: Positive likelihood ratio; LR-: Negative likelihood ratio; DOR: Diagnostic odds ratio; ROC: Receiver-operating curve; IR: Institutional Review; MUMS: Mashhad University of Medical Sciences; PPV: Positive predictive value; NPV: Negative predictive value; Apgar score: a scoring system used to assess the health of newborns immediately after birth; T-test: Student's t-test; Mann-Whitney test: a nonparametric test for comparing two independent groups; Cohen's kappa coefficient: a statistical measure of inter-rater agreement between two raters.
Introduction
A cesarean section, which involves laparotomy followed by hysterotomy, is a common procedure with a multiple cesarean rate estimated at 1 in 6,000 pregnancies [1,2]. However, one of the main complications of multiple cesareans is the development of adhesions, which are fibrous bands that form between organs and the abdominal walls [3].
Laparotomy is a major contributor to the incidence of intra-abdominal adhesions, with an estimated 32% rate due to cesarean section observed among Iranian women [4,5]. Adhesions can lead to a range of complications, including infertility, bowel obstruction, and urinary tract injury [6-8]. Surgeons must therefore predict adhesions in patients before surgery to plan a multidisciplinary team of surgeons and inform the patient of the potentially high risk of complications. Dynamic ultrasound techniques, such as transabdominal or transvaginal sonography (TVS), are safe, well-tolerated, and inexpensive methods that can be used to predict adhesions before surgery [9]. Therefore, the purpose of this study was to explore and compare the diagnostic accuracy of the sliding sign technique, when using abdominal and TVS, in predicting intraabdominal uterine adhesions in pregnant women with a history of previous cesarean section.
Material and method
Study design
This multi-center prospective study was conducted at Qaem and the Imam Reza Hospital, Mashhad, Iran. The protocol of the current study was approved by the Research Ethics Committee of Mashhad University of Medical Sciences (code: IR.MUMS.MEDICAL.REC.1399.611).
Participants
In this study, between 2020 and 2021 we recruited pregnant women (≥ 36 weeks’ gestation) with a history of at least one cesarean section, who were candidates for elective cesarean. The study protocol was described to all women who fulfilled the inclusion criteria, and an informed consent form was obtained from each patient. Exclusion criteria were patients with a known history of collagen diseases or placenta accreta spectrum.
Ultrasound examinations
Abdominal ultrasound
An ultrasound examination of the patient was performed in the supine position. The patient was not asked to empty the bladder unless the patient felt uncomfortable with the full bladder. Abdominal ultrasound was performed by a single sonographer (maternal-fetal medicine specialist). The used ultrasound machine was Philips, affinity 70, using a curved abdominal transducer C6 -2. At the level of the umbilicus, bilateral to the midsagittal line, the probe was positioned vertically, and the patient asked to perform a deep inhalation and exhalation. The movement of the myometrium's outer surface relative to the abdominal fascia's inner surface was evaluated by at least one centimeter of displacement. If the patient had uterine displacement (positive sliding sign), she was considered in the negative adhesion group; and in the absence of displacement (negative sliding sign), she considered in the positive adhesion group (Video 1). During the ultrasound procedure, the film was recorded, which could also be reviewed after. The sliding sign can be searched in a few seconds, and could be performed simultaneously with other third-trimester ultrasounds.
Transvaginal sonography (TVS)
The probe was placed in the anterior vagina to assess the vesicouterine pouch, and the movement between the vesicouterine fold and the anterior uterine face was assessed. The fundus of the uterus could be mobilized by palpation if necessary. The sliding sign was positive if the anterior uterine wall glided smoothly over the posterior abdominal wall. Virgins and patients who declined to undergo TVS were excluded from the study (Video 2).
Evaluation at the cesarean procedure
The presence and degree of uterine adhesion was evaluated by two already trained surgeons. The decision of the trained surgeon was the golden standard. Grading of the uterine adhesion was as follows: degree 0 = equal to no adhesion, grade 1= minimal and very thin adhesion, grade 2 = high thickness adhesion, and grade 3 = severe adhesion (no cleavage plane between the abdominal wall and uterus and viscera). To prevent bias, surgeons were blinded to the ultrasound scan results, and the sonographer was blinded to the surgical finding. A second surgeon would be consulted if there was any doubt about the degree of adhesion.
Demographics and related data
Demographic characteristics and other related data were recorded such as gestational age at recruitment, past pregnancy history, number of previous cesarean sections, time from skin incision to uterine incision (incision time [minutes]), time from skin incision to delivery (delivery time [minutes]), and infant Apgar scores (1st and 5th minute) at birth.
Statistical analysis
Descriptive statistics for the continuous variables are presented as mean and standard deviation and for categorical variables as frequencies (%). Data were analyzed to determine the accuracy of the preoperative TVS and abdominal negative sliding sign in the prediction of uterine adhesions in terms of sensitivity, specificity, positive (PPV) and negative (NPV) predictive values, positive (LR+) and negative (LR–) likelihood ratios and diagnostic odds ratio (DOR). These analyses were then repeated for each compartment separately, along with the analysis of receiver-operating curve (ROC) characteristics. When appropriate, Student’s T or Mann-Whitney U test were used. Cohen's kappa coefficient test was used to compare abdominal and transvaginal ultrasound methods in predicting uterine adhesion before surgery. We used the statistical significance for the prediction of uterine adhesions using the negative sliding sign. A p value of <0.05 was considered statistically significant. Statistical analysis was performed with IBM SPSS Statistics v. 26 (IBM Corp., Armonk, NY, USA).
Results
Demographic and past pregnancy history
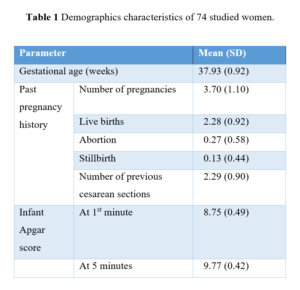
A total of 74 women were enrolled in this study, with a mean age of 32.43 ± 4.92 years. The demographic characteristics of the study population are provided in Table 1, including gestational age of pregnancy, number of pregnancies, number of live births, abortions, stillbirths, number of previous cesarean sections, and infant Apgar score at 1 and 5 minutes at birth.
Uterine adhesion evaluation
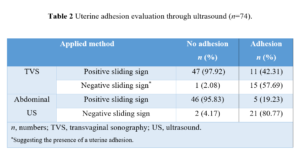
Uterine adhesions were noted during surgery in 26/74 (35.14%) patients. Among them, adhesions were mild in 14 cases, moderate in 7 cases, and severe in 5 cases. Evaluation of uterine adhesion using TVS and abdominal ultrasound is presented in Table 2. The number of suspected uterine adhesions diagnosed by TVS and abdominal ultrasound (negative sliding sign) were 16/74 (22%) and 23/74 (31%), respectively.
Comparison of cesarean outcomes based on adhesion
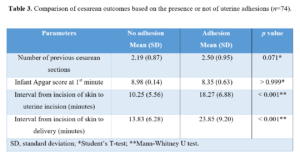
There were no significant differences between positive and negative uterine adhesion groups when comparing the number of past cesarean sections (p=0.071). First minute infant Apgar score did not differ among groups (p>0.999). The mean interval time (minutes) from the incision on the skin to the uterine incision and delivery was significantly higher in the adhesion group (p<0.001) (Table 3).
Accuracy of preoperative transvaginal and abdominal sonographic negative sliding sign in the diagnosis of uterine adhesions
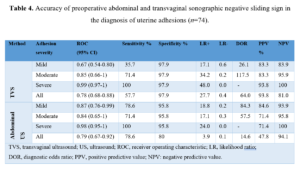
The sensitivity of the preoperative TVS negative sliding sign in the prediction of uterine adhesion was 57.7%, and the specificity was 97.9%. For abdominal ultrasound, the negative sliding sign showed a 78.6% sensitivity in the prediction of uterine adhesion and an 80% specificity (Table 4). For the comparison of abdominal and transvaginal ultrasound methods in the prediction of uterine adhesion prior to surgery, we used Cohen's kappa coefficient test, which was 0.41 and was statistically significant (p <0.01), which indicates a moderate level of agreement between the two methods.
Discussion
While the use of the sliding sign technique during real-time dynamic ultrasound is well established in the management of endometriosis [10-13], there have been inadequate studies evaluating its prediction of uterine adhesions related to multiple cesarean sections. In a study by Shu et al. [14] regarding 112 pregnant women with a history of multiple cesarean sections, the sliding sign technique predicted abdominal uterine adhesions with a sensitivity of 53.3%, a specificity of 80.4%, a PPV of 29.6%, and a NPV of 91.8%. However, the sliding sign technique only detected half of the adhesions. The inter- and intra-observer variability Cohen's kappa coefficient was 0.43 and 0.45, respectively, indicating the unreliability of the technique. A kappa value of 0 indicates no agreement, and 1 indicates perfect agreement. In general, a kappa value between 0.4 and 0.6 represents moderate agreement, while a kappa value between 0.6 and 0.8 represents substantial agreement. A kappa value greater than 0.8 indicates almost perfect agreement. Bukar et al. [15] evaluated the power of the abdominal sonographic sliding sign technique in predicting intraabdominal adhesions in 67 pregnant women in the third trimester of pregnancy. They categorized adhesions as mild, moderate, and severe, and evaluated the technique's power in each category. While the overall sensitivity and specificity of the technique was 100%, the sensitivity and specificity were 5% and 82.98%, respectively, in moderate intraabdominal adhesions, and 25% and 98.41%, respectively, in severe cases. The Cohen's kappa coefficient of the study was 0.58. Baron et al. [16], who were pioneers at introducing the sliding sign technique in pregnant women, found a sensitivity of 76.2% and specificity of 92.1%. The inter- and intra-observer variability Cohen's kappa coefficient was 0.52 and 0.77, respectively. Nirumanesh et al. [17] evaluated among third trimester pregnant women the accuracy of the abdominal sliding sign in detecting intra-abdominal adhesions. They reported that abdominal ultrasound could be an easy diagnostic method for predicting intra-abdominal adhesions, especially in severe cases.
The present study investigated the predictive value of the negative sliding sign technique in detecting uterine adhesions related to multiple cesarean sections. Our results showed that the negative sliding sign using the TVS method for diagnosing uterine adhesion displayed an overall sensitivity of 57.7%, specificity of 97.9%, positive LR 27.6, negative LR 0.4, PPV 93.8% and NPV 81%. A negative sliding sign upon abdominal ultrasound showed an overall sensitivity of 78.6%, specificity of 80%, positive LR 3.93, negative LR 0.1, PPV 47.8% and NPV 94.1%.
Although ultrasound is safe, non-invasive, and well-tolerated, operator dependency is one of the main limitations of this method. To minimize operator bias, the ultrasound probe can be positioned on the scar location or lateral to the scar and the deep breath technique can be used. The deep breath technique was utilized in the present study [15,16].
The strength of this study lies in the large sample size, evaluation of sliding sign accuracy based on adhesion severity, and determination of inter- and interobserver variability. The main limitation of the study is the inability to determine the quality of the deep breath in the patient, which could affect the accuracy of the sliding sign technique.
Conclusions
In conclusion, the findings of this study suggest that abdominal ultrasound has an overall higher sensitivity compared to transvaginal ultrasound in predicting intra-abdominal uterine adhesions in pregnant women with a history of cesarean sections. However, in this regard, transvaginal ultrasound exhibits a higher specificity when compared to abdominal ultrasound.
Contributors: All the authors have made substantial contributions to the conception, design of the work, or the acquisition and analysis or interpretation of data. They have participated in drafting the manuscript and approved the version to be published.
Data availability: Data are available on reasonable request to the corresponding author.