Most studies on the use of testosterone in postmenopausal women have been based on DSM-4 terminology [1], and patients have been diagnosed with hypoactive sexual desire disorder (HSDD) rather than female sexual interest and arousal disorder (FSIAD), the concept introduced in DSM-5. In DSM-4, HSDD is defined as a “persistent or recurrent deficiency or absence of sexual fantasies and desire for sexual activity that causes marked distress or interpersonal difficulty.” It is estimated that HSDD affects approximately 1 in 10 women of all ages and is the most prevalent female sexual dysfunction in postmenopausal women [2]. Low sexual desire is associated with emotional or psychological distress, low self-esteem, and depression [2]. Therefore, HSDD may result in significant impairment in quality of life.
The most commonly used and effective treatment for testosterone deficiency is testosterone replacement therapy. Its non-oral formulations, such as transdermal patches or gels/creams, have been extensively studied in clinical trials, systematic reviews, and meta-analyses. According to recent studies, in postmenopausal women transdermal testosterone significantly improves sexual function with fewer adverse lipid effects compared with oral formulations [3]; in men with hypogonadism, steady transdermal administration restores normal testosterone levels and consistently improves hypogonadal symptoms [4]. Several studies have demonstrated that, in surgically menopausal women (SMW), a 300 µg/day testosterone patch significantly increases satisfaction with sexual activity [5,6].
Similar results have been reported in studies that analyzed testosterone patches in naturally menopausal women (NMW) [7]. Moreover, in surgically menopausal women (SMW) and NMW not undergoing estrogen therapy, the available data demonstrate that the use of transdermal testosterone increases the number of satisfying sexual encounters compared with the placebo group [8]. It is important to underline the dose–response effect, as lower doses of testosterone (150 µg per day) do not provide significant benefits [7]. According to recent studies, testosterone also significantly improves sexual desire in both surgically menopausal women [5] and naturally menopausal women [9]; the data demonstrate improvements in sexual arousal, orgasm, sexual responsiveness, sexual self-image, as well as a reduction in sexual concerns [5,7]. Moreover, the use of testosterone consistently reduces personal distress associated with low sexual desire [7,9]. It is important to acknowledge that all studied doses administered by the transdermal route have led to a significant decrease in distress; therefore, it is reasonable to state that distress reduction is dose-related [8].
The clinical relevance of transdermal testosterone treatment was demonstrated in the study by Kingsberg et al. (2007), who, in a randomized, placebo-controlled trial involving 132 surgically postmenopausal women, confirmed that 6 in 10 women who received testosterone reported meaningful treatment benefits, including an increase in the frequency of satisfying sexual activity, increased sexual desire, and a decrease in distress [10].
Testosterone therapy is well tolerated in both surgically and naturally menopausal women [5,7], and discontinuation rates due to adverse events are generally low [7]. The most commonly reported androgenic adverse events include unwanted hair growth [2,6], acne [2], as well as “anecdotal” virilization (clitoromegaly) when supraphysiological doses are used [11]. It should be noted that testosterone patches generally aim to achieve physiological levels, and no cases of virilization have been observed.
In conclusion, testosterone therapy, particularly via the transdermal route, consistently demonstrates statistical and clinical improvements in sexual desire, satisfying sexual activity, and reductions in personal distress associated with low desire in both surgically and naturally menopausal women. While generally well tolerated, androgenic adverse events, primarily unwanted hair growth, are observed at higher hormone doses. Long-term safety data spanning up to four years, based on various laboratory-tested parameters, generally show no significant adverse effects.
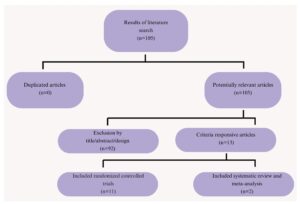
A detailed summary of the role of testosterone therapy in the lives of postmenopausal women is presented in the systematic review published in this issue of EGO. The review entitled “Efficacy and safety of testosterone treatment in postmenopausal female sexual interest and arousal disorder” consolidates key information regarding the utility of testosterone in addressing low sexual desire disorder in postmenopausal women, emphasizing its established efficacy and generally favorable safety profile.