Introduction
Women may experience increased vaginal or peri-vaginal secretion in connection with sexual arousal, and some report an additional increase specifically associated with orgasm, commonly referred to as female ejaculation.
Female ejaculation has been described in both general erotic literature and professional gynecological literature. Some women report that increased secretion occurs only during certain orgasms, whereas others experience it more frequently. This article distinguishes between three types of secretion: 1) natural lubrication of the vaginal walls during sexual arousal, described by Masters and Johnson as an ultrafiltrate of blood plasma (vaginal smear); 2) a whitish, viscous fluid, typically only a few milliliters in volume (paraurethral secretion) originating from Skene’s glands; and 3) a larger volume of thinner fluid, often referred to as “squirting” in the English-language literature [1-3].
Rubio-Casillas’ biochemical analyses from 2011 describe squirting and paraurethral secretion as two distinct fluids with separate origins and mechanisms [4]. A Japanese study from 2022 visualized squirting in five women known to be able to squirt. Their bladders were emptied by catheterization and then filled with a mixture of indigo carmine and saline. All five secretions following sexual stimulation were blue, confirming the bladder as the source of the fluid. Prostate-specific antigen (PSA) was detected in fluid from four of the five women [5]. Taken together, the available evidence suggests that female ejaculation is usually a mixture of paraurethral secretion and urine from the urinary bladder, although it may occasionally originate from only one of these sources.
The literature reports widely varying estimates of the prevalence of female ejaculation [2]. Earlier studies often made little distinction between paraurethral secretion and squirting, and reports of high frequency are largely based on women’s subjective experiences [3]. The most cautious conclusion at present is that the prevalence of ejaculation among sexually active adult women remains uncertain, as do the conditions under which it occurs.
In this study, we interviewed a group of female medical students at the University of Oslo in January 2023. The aim was to explore different aspects of the female orgasm, including stimulating and triggering factors, distinctions between types of secreted fluids (vaginal smear, squirting, and paraurethral secretion), and the frequency, volume, and consistency of these secretions. The study also collected information on participants’ backgrounds, as well as their emotions and thoughts related to sexual experiences. The participants constituted an anonymized and voluntary group of female medical students with varying levels of basic knowledge of female anatomy and physiology.
Method
The study included 53 female medical students at the University of Oslo. All individual in-depth interviews were conducted by HFA, who was also responsible for recruiting participants. The interviewees were aged 19–29 years and represented students from the first to the sixth year of study during the autumn semester of 2022. The medical program at the University of Oslo has 120 places per cohort, with admissions in both August and January. In total, 1,425 students were enrolled in medicine in autumn 2022, of whom 1,022 (72%) were female. Thus, the interviewees represented approximately 5% of the female medical students that semester.
All participants were medical students, as this group was expected to feel comfortable discussing their bodies and sexuality. In addition, they were assumed to have greater understanding of, and interest in, female anatomy and physiology than women of the same age in the general population. It was also considered likely that participants would feel a degree of trust toward the interviewer as a fellow student. Women of all sexual orientations, with sexual experience either alone or with one or more partners, were included. Transwomen were excluded, as the study focused on orgasm in biological females.
Participants were recruited through informal social interactions at Domus Medica, the main building for medical students on the Oslo campus. These interactions included lunch breaks in the canteen, student associations such as women’s choirs, and students studying in the faculty library or study halls. Invitations were delivered verbally or by text message and were described simply as “interviews about female sexuality and orgasm.” No further details were provided, apart from an estimated duration of 20 minutes. Only three women declined participation, all citing lack of time.
The interviews were conducted in January 2023 at Domus Medica or Rikshospitalet (Oslo University Hospital). Only the interviewer and the participant were present. To ensure anonymity, no interviews were conducted by telephone or video, and no recordings were made.
The interview questions were planned as a structured guide (see Supplementary Information), but the outline was not shared with participants. The aim was to allow women to speak freely, and follow-up questions varied between interviews. There was no fixed duration, although the average interview lasted 26 minutes. Responses were recorded in real time on a laptop and subsequently transcribed by hand into a separate notebook with fixed pages. Participants’ names were not recorded.
No questions were asked about contraception, sexually transmitted diseases, pregnancies, induced abortions, or childbirth, in order to avoid any perception of moral judgment. Instead, participants were invited to discuss factors or experiences—positive or negative—that might have influenced, or were still influencing, their sexuality. Female genital mutilation, medication, and genital surgery were mentioned only as examples. Sexual debut, whether alone or with a partner, was defined as the “first conscious stimulation for pleasure.” No requirements were imposed regarding the type of sexual activity or self-stimulation.
Results
Age and background
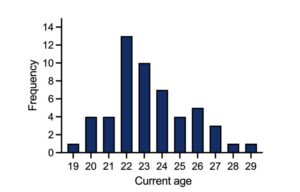
Fifty-three female medical students were interviewed. The participants were aged 19–29 years1, with a mean age of 23.3 years and a median of 23 years (Figure 1). The women were not asked which year of their studies they were in.
1 In Norway, age is reported as the number of completed years since birth (e.g., a woman is considered 21 years old from her 21st until her 22nd birthday). Accordingly, the reported ages may underestimate the chronological age by approximately six months on average.
Forty-seven of the 53 interviewees were ethnically Norwegian and had an upbringing influenced by Western and what they described as “typically Norwegian” culture. The remaining six were of Balkan or Asian origin and had a cultural upbringing influenced by Islam, Buddhism, or Hinduism. All six had completed most of their schooling in Norway. Seven of the 53 interviewees identified themselves as devout Christians. Thirty-seven of the 53 interviewees reported an open-minded culture around sexuality during their upbringing and adolescence, while seven reported that this subject was highly taboo both at home and among their peers. The remaining nine described their culture as moderately open-minded.
Sexual orientation
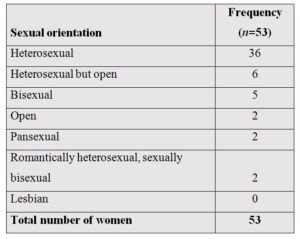
Thirty-six of the 53 interviewees identified themselves as heterosexual (Table 1), and an additional six described their orientation as “heterosexual but open.” Of the 36 women who identified as heterosexual, 15 had one or more previous female sexual partners.
Two individuals identified as “open,” stating that they found the question difficult to answer. Two others reported that they were romantically heterosexual but sexually attracted to both genders (sexually bisexual). Of the remaining interviewees, five identified themselves as bisexual and two as pansexual. None identified as lesbian or queer (Norwegian: lesbisk or skeiv).
Sexual debut
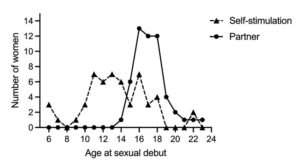
Sexual debut alone, defined as the first conscious self-stimulation for pleasure, occurred at a mean age of 13.4 years, with a median of 13 years. Sexual debut with a partner, defined as the first stimulation for pleasure with a partner, occurred at a mean age of 17.3 years, with a median of 17 years (Figure 2).
The questions did not specify the type of intercourse or stimulation, and sexual debut with a partner was deliberately not defined as penetrative vaginal and/or heterosexual intercourse.
Sexual partners
All 53 women reported sexual experience both with self-stimulation and with one or more partners. In addition, all had experience with one or more male partners. Fifteen individuals had experience with one or more female partners.
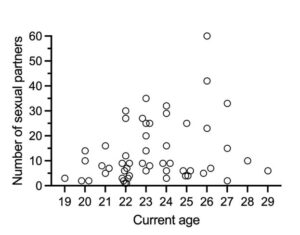
The total number of sexual partners throughout a woman’s lifetime ranged from one to 60, with a mean of 13.4 and a median of 9 partners per woman (Figure 3). A partner was defined as a person with whom a woman had one or more sexual interactions, without specification of the type of interaction. The women were allowed to define the term “sexual partner” individually.
As expected, the number of sexual partners increased with age from 19 to 29. A simple linear regression showed an increase of 1.45 partners per year over these eleven years, from seven partners at age 19 to 21 partners at age 29. Since a few of the older women reported a high number of partners (Figure 3), a more robust regression method using rank was also applied. This showed an increase of 0.8 partners per year, from six partners at age 19 to 14 at age 29.
The group of six students with other religious and/or cultural backgrounds and the seven who identified as devout Christians reported sexual behavior similar to the rest of the sample. The median age at first stimulation for pleasure with a partner was 18 years in both groups. The median number of previous sexual partners was seven in the first group and six in the second, although both distributions showed wide variability.
Negative experiences
The interviewees were asked about personal factors that could affect their sexual experiences positively or negatively. Gender confirmation surgery, genital mutilation, and medication were the only examples provided by the interviewer. Nine individuals spontaneously reported experiencing sex without consent one or more times. They reported that this had, for a prolonged period, restricted or was still restricting their sexual lives and physical and mental health. These interviewees represent 17% of the study population.
Three women reported decreased libido during periods of oral contraceptive use, with improvement after discontinuation. A similar pattern was reported by three individuals using antidepressants. One interviewee reported increased libido after treatment with stimulant medication for Attention-Deficit/Hyperactivity Disorder (ADHD). Five individuals had been diagnosed with vaginismus and reported pain during vaginal intercourse at the time of the interview. Two additional women described similar pain without a formal diagnosis.
Orgasm
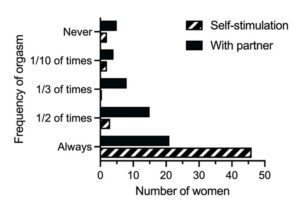
Forty-seven of the 53 interviewees had experienced orgasm both through self-stimulation and with one or more partners. Five had experienced orgasm only through self-stimulation, and one had never experienced orgasm. Forty-six interviewees reported always achieving orgasm through self-stimulation, whereas only 21 reported always achieving orgasm with a partner.
Fifty women reported clitoral stimulation as the trigger for orgasm. Penetrative stimulation with fingers, penis, or sex toys was reported by 16 interviewees, of whom four experienced multiple orgasms. Fifteen interviewees reported orgasm through stimulation around the vaginal opening, while two had only experienced orgasm through oral stimulation of this area.
Several factors were described as helpful in achieving orgasm, most commonly trust in a partner. Other factors included breast stimulation, body contact, and good communication.
Eleven interviewees who had experienced both clitoral and penetrative orgasm described them as different. Clitoral orgasm was described as localized and superficial, while penetrative orgasm was described as deeper and more intense, sometimes involving the whole body. All interviewees reported genital sensitivity immediately after orgasm. Forty-six interviewees reported involuntary vaginal contractions during orgasm, and 18 reported uterine contractions. Pulsation of the clitoris was described by 18 interviewees.
Fifty-two interviewees reported exclusively positive feelings during orgasm. Twenty-four described a tingling sensation and warmth spreading through the body, and 41 reported a general sense of lightness, with 12 describing this as euphoria.
Ejaculation
Twenty-six of the 53 interviewees reported experiencing ejaculation just before, during, or immediately after orgasm, with 10 describing it as a visible expulsion of fluid (“squirting”). Ejaculation was defined as an increase in genital secretion associated with orgasm, distinct from normal lubrication.
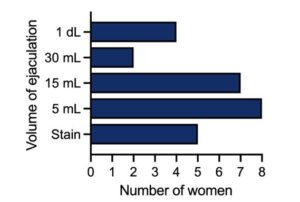
Seven partners of the 10 women who reported visible expulsion also confirmed observing the fluid. Some women who did not report visible squirting described a noticeable increase in fluid, such as wet bedding. One interviewee stated that it was “enough to make me change the bedding,” while five others described a wet area with a diameter of 5–6 cm. Reported quantities ranged from approximately 5 mL to 1 dL. The remaining 27 interviewees did not report a noticeable increase in secretion.
Twenty-four women had experienced ejaculation with a long-term partner, and 14 of these had also experienced it during self-stimulation. The remaining two reported experiencing it only during self-stimulation.
Twenty interviewees reported that clitoral stimulation led to orgasm with ejaculation. Eight reported that ejaculation depended on G-spot stimulation with fingers, penis, or sex toys, sometimes in combination with other forms of stimulation. Oral stimulation in the vulvar area and anal penetration were also mentioned.
Two interviewees described the ejaculate as a whitish, thicker secretion. One of these also reported experiencing, on other occasions, a larger volume of less viscous fluid consistent with squirting, distinguishing between the two. The remaining 24 interviewees described the fluid as clear and watery.
All interviewees noted that the likelihood of ejaculation increased with longer duration of stimulation. Nine reported that it most often occurred after the third or fourth consecutive orgasm.
Of the 26 interviewees who had experienced ejaculation, five reported it only once, while three reported experiencing it with every orgasm.
Discussion
The 53 female medical students who were interviewed do not constitute a strictly random sample of all female medical students at the University of Oslo in the fall of 2022. Nevertheless, the method of selecting interviewees likely resulted in an almost random sample of those who remained in Domus Medica between lectures, courses, and clinical teaching. Only three of the women approached declined participation.
Even so, the sample may overrepresent how liberated Norwegian women are in their sexuality, as this group consists of highly educated and independent women. They are also socially active, spending time at Domus Medica or in student associations. From experience, students engaged in these activities tend to be more outgoing, open, and curious, and may therefore have had more varied experiences, including sexual experiences, than is typical for women of the same age.
Despite these limitations, many of the responses provide valuable insight into the experiences and attitudes of Norwegian female medical students, and possibly, in some areas, into those of Nordic women in this age group at the present time.
All participants were asked about their sexual orientation (“Hva er din egen seksuelle legning”), and the responses are presented in Table 1. It is notable that none identified as lesbian or queer. Several explanations are possible, one of which was mentioned by multiple participants: they were still exploring their sexuality and did not wish to label it. Instead, terms such as “pansexual”, “bisexual”, or “open” were used.
The median age of sexual debut alone, defined as the first conscious self-stimulation for pleasure, was 13 years (Figure 2), with 32 participants reporting an age between 10 and 15 years. This suggests that first sexual experiences often occurred close to sexual maturity. Age at menarche has remained relatively stable in Norway at approximately 13.25 years (SD = 1.04) since 1950 [6]. Five participants reported first self-stimulation occurring in childhood, between six and nine years of age. This phenomenon was described as early as 1953 by Kinsey [7].
All 53 women reported experience with male partners. As only 15 had experience with female partners, most likely had a male partner as their first sexual partner. The median age of first sexual intercourse was 17 years; 47 participants reported first intercourse between the ages of 15 and 19, while five were older (Figure 2). These ages are slightly higher than those reported in population-based surveys in Nordic countries [8].
Thirty-two participants reported between one and ten lifetime sexual partners (Figure 3), sixteen reported between 11 and 30 partners, and five reported more than 30 partners. Only a few participants provided approximate numbers; most reported exact figures, sometimes after consulting notes on their mobile phones. There are limited data for comparison, either from Norway or other countries. In Walløe’s interview study from 1974, the interviewers included female medical students aged 22–24 years [9], who are now retired physicians. Informal follow-up conversations suggest that, although they were sexually active at the time, they typically reported only a small single-digit number of partners—substantially lower than those reported in the present study. There is limited information on when these changes in sexual behavior occurred over the past fifty years. Contraceptive methods, including hormonal contraception and IUDs, as well as access to induced abortion, have been available throughout this period.
Given that 48 of the 53 participants reported regularly experiencing orgasm through self-stimulation, and that 46 always achieved orgasm in this context, whereas only 20 consistently did so with a steady partner, difficulties with orgasm may be related to partner interaction. Several participants highlighted factors such as trust and emotional connection as important for achieving orgasm with a partner. Similar factors, including intimate kissing and relationship satisfaction, have been reported in an American study from 2018 [10]. However, one participant noted that orgasm was easier to achieve with a stranger than with a regular partner, illustrating the variability of sexual experiences.
Only two participants described a secretion consistent with paraurethral secretion. They characterized it as “thick, thicker than water, whitish and/or gray, and only a few drops of fluid.” This was not described as a squirting mechanism, but rather as a steady flow observed by a partner or as a stain on bedding or underwear. These experiences were reported fewer than ten times in their lifetime and typically occurred after prolonged stimulation. One of these participants also reported experiencing squirting and was able to distinguish clearly between the two phenomena. She described differences not only in volume and consistency, but also in subjective experience. Squirting was described as “a pressure, different from the pressure of urination, finally releasing after building up for a long time, followed by a feeling of great satisfaction,” whereas paraurethral secretion was often not noticed at the time and was instead identified by the partner afterward. These descriptions support the hypothesis that female ejaculation may involve a mixture of urine and paraurethral secretion, while also suggesting that each may occur independently.
The reported volume of squirting ranged from a few milliliters to larger amounts resulting in visible wet spots on bedding, with some participants estimating up to one deciliter. These estimates were often approximate, as participants noted difficulty in assessing volume. Nevertheless, the description of a larger volume of clear, thin fluid is consistent with previous reports of squirting [2].
None of the participants reported feeling ashamed of ejaculation at the time of the interview, aside from practical concerns such as needing to change bedding. However, four reported initial embarrassment when first experiencing it at a younger age, often due to uncertainty about what it was. Some participants also mentioned concern about how a new partner might react. All agreed that ejaculation itself contributed little additional pleasure beyond orgasm, although several described a sense of satisfaction related to bodily exploration and intimacy. Some also noted that their partners found the experience pleasurable.
Eleven participants who had experienced both clitoral and penetrative orgasms described them as distinct. Clitoral orgasm was typically described as localized and superficial, whereas penetrative orgasm was described as deeper, more intense, and sometimes involving the whole body. One participant described it as “almost as if all the muscles in the entire body, both superficial and deep, were rhythmically contracting.”
Participants were also asked to describe their physical and mental experience of orgasm. All 52 who had experienced orgasm reported exclusively positive sensations during the event itself, regardless of emotions before or after. Twenty-four described a tingling sensation and warmth spreading from the lower abdomen throughout the body, sometimes reaching the fingertips and toes; two noted that this sensation was particularly intense in the earlobes. A general sense of lightness was reported by 41 participants, with 12 comparing this sensation to euphoria.
In conclusion, more than one third of females in their 20s regularly experience ejaculation in stable relationships. Unlike orgasm itself, ejaculation provided little additional pleasure.
Author contributions
Hijab Fatima Ali planned the interview topics and study protocol, conducted all interviews, performed the initial analysis and interpretation of the results, and drafted the manuscript. Lars Walløe contributed to study design, data interpretation, and critical revision of the manuscript.
Data availability
The primary data from the interviews are not generally available but are kept handwritten in a notebook with fixed pages. Copies may be made available to researchers who can understand Norwegian.