Introduction
Conjoined twins result from incomplete division of the embryonic disc occurring after the 13th day of gestation [1]. The first prenatal diagnosis of conjoined twins by ultrasound was reported in 1976 by Wilson at 35 weeks of gestation [2,3]. Since then, diagnostic capabilities have improved substantially, allowing detection as early as seven weeks of gestation [4,5].
The prevalence of conjoined twins ranges from 1 in 50,000 to 200,000 live births [4], making this condition one of the rarest congenital anomalies. There is a marked female predominance, accounting for approximately 70% of cases [4]. The prognosis remains poor: 40%–60% of conjoined twins are stillborn, and approximately 35% of live-born infants do not survive beyond the first day of life [6,7].
Prognosis depends on the site of fusion, the type of conjoined twins, the extent of shared organs, and the presence of associated malformations. Several classification systems have been proposed, with Spencer’s classification being the most widely adopted. According to this system, conjoined twins are categorized as either ventrally joined—accounting for approximately 87% of cases, with fusion occurring along the anterior midline—or dorsally joined, comprising the remaining 13%, with fusion arising from the neural tube [8].
The most frequently encountered types of conjoined twins include thoracopagus (28% of cases), thoraco-omphalopagus (18.5%), omphalopagus (10%), heteropagus (10%), and craniopagus (6%). Less common forms include pygopagus, rachipagus, ischiopagus, and cephalopagus [7-9]. There are no known cases of conjoined triplets or quadruplets [2,3]. However, some reports describe triplet pregnancies in which two of the fetuses are conjoined [10].
It has been repeatedly reported in the literature that early diagnosis is essential to rapidly establish prognosis and to offer appropriate management, including continuation of the pregnancy or medical termination of pregnancy [11]. However, this diagnosis is not always straightforward [12]. Surgical management remains a major challenge. The first successful separation of conjoined twins was performed in the 17th century by Johannes Fatio in Switzerland in twins joined at the umbilicus [13].
Currently, only a limited number of pediatric surgical teams have the expertise to perform separation procedures in conjoined twins, and only in the absence of severe associated malformations. When prenatal ultrasound reveals major anomalies, medical termination of pregnancy (MTP) should be considered.
Case presentation
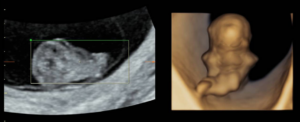
A 33-year-old patient, gravida 1 para 0, presented for a routine examination and dating ultrasound on 06/20/2024. The estimated gestational age was 8 weeks + 6 days. She had no relevant medical history. Her family history was notable for a cousin with trisomy 21. The diagnostic assessment was performed using transabdominal and transvaginal ultrasonography, complemented by three-dimensional (3D) ultrasound. The initial evaluation occurred during a routine first-trimester scan for pregnancy dating at 8+6 weeks of gestation. Ultrasound examination revealed a 23 mm embryo with an enlarged head (Figure 1A). A single gestational sac with two yolk sacs was identified, consistent with a monochorionic–monoamniotic twin pregnancy (Figure 1B).
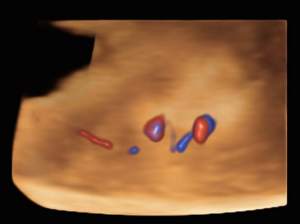
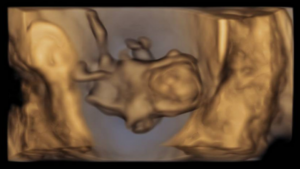
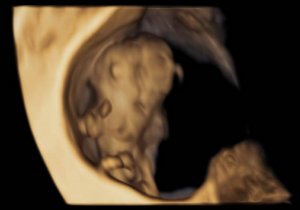
The ultrasound images demonstrated a single spinal column, two stomachs, and two hearts (Figure 2A). Two fused abdomens were observed, along with subcutaneous edema measuring 2.0 mm and 2.1 mm (Figure 2B). In addition, two pairs of moving legs were identified (Figure 2C). The trophoblast was located anteriorly, and a single corpus luteum was observed in the left ovary. Two follow-up examinations were required at 9 and 10 weeks of gestation to establish the diagnosis. At 9 weeks of gestation, the 3D ultrasound images lacked sufficient clarity for a definitive diagnosis (Figure 3). At 10 weeks of gestation, color Doppler imaging demonstrated two distinct cardiac activities, indicating the presence of two separate circulatory systems (Figure 4A). Three-dimensional imaging further revealed the face of one of the conjoined twins and confirmed the presence of two umbilical cords (Figure 4B).
Once the diagnosis was confirmed, a discussion regarding the pregnancy prognosis was held with the couple. Given the poor prognosis, they opted for medical termination of pregnancy (MTP). At 10+3 weeks of gestation, the patient was admitted for MTP. A mifepristone/misoprostol protocol was administered under epidural anesthesia. Complete trophoblastic retention required non-aspirative curettage. No hemorrhage was observed. Samples were sent for pathological examination (trophoblast and fetuses), and a skin biopsy was obtained for genetic karyotype analysis.
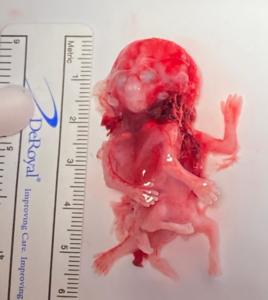
Karyotype analysis and fetal autopsy performed by anatomical pathology yielded the following findings: “External examination (Figure 5): male conjoined twins classified as cephalopagus, with a combined weight of 9 g. The twins were fused dorsally, extending from the cranial vault to the pelvis. A single skull was present, with two distinct faces. One face exhibited a proboscis and a single ocular globe containing two irises. A total of four limbs were identified. Both fetuses presented with anal atresia. No internal examination was performed in accordance with the parents’ wishes.”
Discussion
Conjoined twinning is an exceptionally rare complication of monozygotic pregnancies, resulting from incomplete separation of the embryonic disc beyond the 13th day of gestation. Classification is based on the site and extent of fusion, which directly influences prognosis. Early antenatal identification is crucial for planning appropriate prenatal care and for considering timely obstetric interventions.
A recent review of the literature identified several relevant studies, including one reporting 20 cases of conjoined twin pregnancies diagnosed between 2016 and 2022, with gestational ages at diagnosis ranging from 10 to 35 weeks and an incidence of cephalopagus twins of 20% [14]. An earlier retrospective study published in 2011 described 36 cases over a 12-year period and reported a cephalopagus detection rate of only 2.8% [15].
In addition, we compiled the complete results of our review (Table 1), summarizing the most recent findings on conjoined twin pregnancies (2000-2024), including gestational age at diagnosis, type of conjoined twins, and reported frequencies of cephalopagus conjoined twins in cohort studies. Notably, our review identified only a single case of conjoined twin diagnosis before 8 weeks of gestation, detected during post–in vitro fertilization follow-up [9].
These findings highlight the significance of our case, as the diagnosis of a cephalopagus conjoined twin pregnancy at 8+6 weeks represents an exceptionally early and clinically relevant observation. This further underscores the critical role of ultrasound in the early identification of severe congenital malformations.
The extent of anatomical fusion observed in this case—characterized by a single head with two faces, two distinct hearts, and a shared vertebral column—rendered surgical separation nonviable and was therefore associated with an extremely poor prognosis. The parents, initially unprepared for such a diagnosis, required time for reflection and additional clarification. A follow-up ultrasound performed one week later allowed further diagnostic refinement. This underscores the importance of maintaining a high index of suspicion and being prepared to re-evaluate imaging findings that appear questionable. Ultimately, after comprehensive counseling regarding prognosis and therapeutic options, the couple elected to proceed with medical termination of the pregnancy.
Conclusion
This case report underscores the critical importance of early diagnosis in sporadic obstetric pathologies. Detection of this rare case of cephalopagus conjoined twins at an early gestational age of 8 weeks and 6 days was made possible through a careful and thorough ultrasound examination. Such early identification likely played a key role in mitigating potential obstetric and psychological complications that may arise from delayed diagnosis.
Abbreviations: 3D: three-dimensional; MTP: medical termination of pregnancy.
Ethical considerations
The couple provided informed consent for the anonymous publication of the data and images related to their medical case.