Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disorder that primarily affects movement. It results from the gradual loss of dopamine-producing neurons in the substantia nigra region of the brain. Although classified as a movement disorder, it also causes motor and non-motor symptoms that worsen over time [1].
The disease was first described in 1817 by the British physician James Parkinson in his work An Essay on the Shaking Palsy [2]. While the exact cause of PD remains unknown, evidence suggests that a combination of genetic and environmental factors contributes to its development [3]. This case report discusses the management of a 33-year-old pregnant woman with autosomal recessive PD, emphasizing the multidisciplinary approach employed and reviewing the limited literature on this topic.
Case report
A 33-year-old gravida 3 para 0 presented for her booking appointment at 15/40 following a planned in-vitro fertilization (IVF) pregnancy. She had been diagnosed with autosomal recessive Parkinson’s disease at the age of 22 due to a gene deletion. Genetic testing confirmed two mutations (PARK2 c.101_102delAG) in the PARK2 (PRKN) gene.
She achieved pregnancy through IVF for unexplained subfertility. Both the patient and her partner underwent pre-IVF genetic testing, and her partner tested negative for carrier status. Given the patient’s history and her preference, an elective cesarean section was planned for 39/40 weeks. Additional reasons for this decision included her reduced muscular coordination and her mental health status at the time, which involved anxiety. She received regular neurological follow-up, attended a pre-anesthesia clinic, and engaged in physiotherapy as part of a comprehensive multidisciplinary approach to her care.
Throughout pregnancy, she continued levodopa therapy as advised by the neurology team. At 38/40, she was admitted because of worsening Parkinson’s symptoms, and her levodopa dose was increased. During this admission, she was also prescribed lorazepam and propranolol to manage worsening symptoms and anxiety. Unfortunately, she developed pregnancy-induced hypertension, which was controlled with beta-blockers.
At 38+3/40, she underwent an uncomplicated elective cesarean section under spinal anesthesia, resulting in the birth of a healthy female baby weighing 3,720 grams. She was discharged on the fifth postpartum day after assessments by a neurologist, occupational therapist, and physiotherapist, with an outpatient neurology appointment scheduled three weeks later.
Discussion
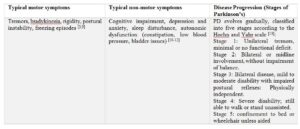
Parkinsonism typically manifests in individuals in their early 60s, making the concurrent occurrence of pregnancy and Parkinsonism rare. Approximately 1% of people over 60 are affected by Parkinson’s disease (PD), making it the second most common neurodegenerative disorder after Alzheimer’s disease [4]. Although the average age of onset is around 60 years, early-onset Parkinsonism, affecting individuals before the age of 40, accounts for only 5–10% of cases, further highlighting the rarity of this coexistence and the management challenges it presents [5,6]. Men are approximately 1.5 times more likely to develop PD [7]. While PD itself is not directly fatal, its complications can reduce lifespan, and advanced disease often leads to significant disability [8]. A brief summary of the typical symptoms and disease progression is provided in Table 1.
Early-onset PD is more likely to have a genetic component than late-onset PD. Several gene mutations have been strongly associated with early-onset forms of the disease. Mutations in the PARK2 (PRKN) gene are the most common cause of juvenile PD (onset before age 20). PINK1, DJ-1, and SNCA have also been linked to early-onset PD, with SNCA mutations being the rarest and typically showing autosomal dominant inheritance. The other gene mutations mentioned above usually follow an autosomal recessive inheritance pattern.
As in the present case, mutation of the PARK2 gene impairs the cell’s ability to clear damaged proteins, leading to neuronal dysfunction. This mutation was first reported in association with PD in 1998 [14]. Because it follows an autosomal recessive pattern, carriers are typically asymptomatic; therefore, the patient’s partner underwent genetic testing before IVF treatment.
Given the rarity of PD during pregnancy and the limited number of documented cases, there is little high-quality evidence to guide standardized management or predict complications. No randomized trials on PD treatment in pregnancy currently exist; most recommendations are based on case series, expert opinion, and general principles of drug safety.
Treatment of PD is primarily symptomatic, as there is no definitive cure. Current management focuses on improving quality of life by addressing individual symptoms. Both pharmacologic and non-pharmacologic approaches are supported by a strong evidence base.
Levodopa, which is converted to dopamine in the brain [15], is considered the gold-standard therapy for most PD subtypes, including during pregnancy. Patients with PARK2 mutations, in particular, have been shown to respond especially well to levodopa [16]. Dopamine agonists such as pramipexole and ropinirole are also used to mimic dopamine activity and help control symptoms related to dopamine deficiency [15]. However, in the context of pregnancy, levodopa remains the first-line and preferred treatment.
Monoamine oxidase-B (MAO-B) inhibitors, including selegiline and rasagiline [15], are not recommended during pregnancy because of limited human data and evidence of potential fetal toxicity in animal studies [17,18]. Amantadine is contraindicated in pregnancy due to documented teratogenic effects [17,18].
Non-pharmacologic options include deep brain stimulation (DBS), which has been shown to improve quality of life by reducing dyskinesia in advanced PD [19,20]. Multidisciplinary care—incorporating physiotherapy, occupational therapy, and dietary support—can also contribute to lifestyle modification and better symptom control [19,21]. In addition, emerging research is exploring neuron replacement through stem cell therapy as a potential future treatment for PD [22].
A multidisciplinary approach involving the general practitioner, neurologist, anesthetist, and obstetrician is recommended—even in the pre-pregnancy phase—to establish both long- and short-term management strategies [6]. Case reports suggest that non-pharmacological measures (physical therapy, occupational therapy, and sleep hygiene), combined with coordinated neurologist–obstetrician care, can be effective in managing Parkinson’s disease during pregnancy [23]. Additionally, patients should be informed and counselled about the potential worsening of symptoms during or after pregnancy [17].
Conclusion and recommendations
In summary, the coexistence of Parkinson’s disease and pregnancy is rare and may carry maternal and fetal risks; however, effective management through a multidisciplinary team approach can support a favorable pregnancy outcome. Levodopa remains the preferred treatment option for Parkinson’s disease during pregnancy. Nevertheless, further research is needed because of the limited literature available on this subject.
Author contributions
All authors contributed to the care and follow-up of the patient and revised and approved the final submitted manuscript.
Patient informed consent
Patient provided informed consent for the publication of the case report.